Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
In China, the malaria elimination program was launched in 2010 with the objective to eliminate this disease by 2020. Large-scale malaria control and elimination actions have been conducted with significant success since inception of the nationwide program. The incidence of locally acquired malaria has declined sharply along with the concomitant decrease of malaria-endemic areas from 762 counties reporting malaria in 2010 to just two counties adjacent to border areas (Yunnan, China-Myanmar and Tibet, China-India) in 2016. In total, 1723 counties (79%) and 134 prefectures (52%) had completed the malaria elimination internal assessment by the end of 2016. The year 2017 was the first year without report of indigenous malaria cases throughout the country. Hence, this chapter is meant to share the lessons learned from malaria elimination in China benefiting countries on the way to malaria elimination.
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
IES, University Montpellier, CNRS, France
Cirad, UMR 17, Intertryp, Campus international de Baillarguet, France
HSM, IRD, CNRS, Univ. Montpellier, France
Li Zhang
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
Jun Feng
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
Jianhai Yin
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
Xinyu Feng
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
Zhigui Xia
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
Roger Frutos
IES, University Montpellier, CNRS, France
Cirad, UMR 17, Intertryp, Campus international de Baillarguet, France
Sylvie Manguin
HSM, IRD, CNRS, Univ. Montpellier, France
Shuisen Zhou*
National Institute of Parasitic Diseases, Chinese Center for Disease Control and Prevention (China CDC), China
National Center for Tropical Diseases Research, China
Key Laboratory of Parasite and Vector Biology, Ministry of Health, China
National Center for International Research on Tropical Diseases, Ministry of Science and Technology, China
WHO Collaborating Center for Tropical Diseases, China
*Address all correspondence to: shuisenzhou@126.com
1. Introduction
Although significant progress on malaria control and elimination has been made worldwide, malaria remains a major public health threat to human beings. According to the World Malaria Report published by the World Health Organization (WHO), a total of 216 million malaria cases were reported worldwide with 445,000 deaths in 2016 [1]. These malaria cases were mainly reported from Africa (90%) and Southeast Asia (7%). With the available intervention tools, several countries have been certified to be malaria-free, and others are in the process of elimination in the foreseeable future [1]. Among others, within the broad objective of worldwide malaria elimination [2], 21 countries have the potential to eliminate malaria by 2020; these are marked as E-2020 countries by WHO [1]. Although some of E-2020 countries were moving forward to achieve elimination goals, 111 have reported an increase of indigenous malaria cases since 2015, and 5 countries2 reported >100 cases in 2016 compared to 2015. World malaria elimination is currently at crossroads [3].
Among the E-2020 countries, China has made a significant progress on malaria elimination. Both the malaria-endemic territories and indigenous cases have decreased dramatically [4, 5, 6]. Furthermore, no indigenous cases were reported in China in 2017. Along with the decrease of indigenous malaria cases, the distribution of Plasmodium species associated to the reported malaria cases had changed as well. Only 2 Plasmodium species, i.e., Plasmodium falciparum and P. vivax, were present prior to the elimination program, but now all 4 human malaria parasites are encountered in China (i.e., P. falciparum, P. vivax, P. malariae, and P. ovale), as well as the simian species P. knowlesi [1, 7, 8, 9, 10, 11, 12]. The predominant Anopheles vectors had also changed over the same period due to environmental changes and anti-malaria interventions. Prior to malaria elimination, 4 main species/complexes of vectors were recorded, i.e., Anopheles lesteri, An. dirus s.l., An. minimus s.l., and An. sinensis (Table 1). Currently, after 7 years of malaria elimination efforts, only 2 species/complexes are recorded to be prevalent, i.e., An. minimus s.l. (mainly An. minimus and An. harrisoni) and An. sinensis. Moreover, the geographic distribution range of An. sinensis has expanded and the proportion increased too [13, 14, 15, 16]. Considering the progress of malaria elimination in China and the challenges still to be met, useful information has been generated which could be shared with the communities working on malaria elimination. This chapter is thus aiming at detailing the strategy of the Chinese national malaria elimination program, current progress, and lessons learned in defeating malaria.
Anopheles species/taxa
Sibling species prevalent in the People’s Republic of China
The national malaria elimination strategy was developed based on the malaria control situation and response to the Global Eradication of Malaria Initiative proposed by the United Nation Millennium Development Goals (MDGs) in September 2000 [5, 17, 18]. The overall strategy comprised specific objectives and key measures taking into account the different epidemiological contexts and diversity of malaria transmission models all over the country. The overall goals of malaria elimination in China were set to achieve zero indigenous cases in the country by 2015, leaving apart the border areas of Yunnan Province with Myanmar and Tibet Autonomous Region with India to achieve complete elimination in the country by 2020.
2.1. Intermediate objectives
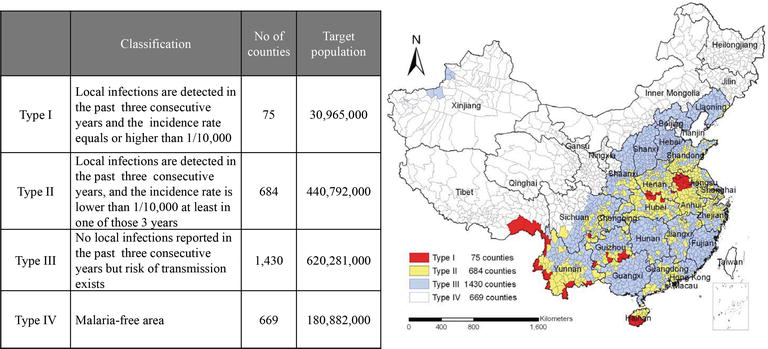
The strategy and key measures for malaria elimination in China were developed in line with the WHO guidelines [19]. However, counties had variable endemicity based on which a classification was established according to the different types of area and intensity of malaria transmission. According to the magnitude of transmission and incidence, all counties were classified into 4 types, including Type I, local transmission and incidence ≥1/10,000 over the past 3 years; Type II, local transmission and incidence <1/10,000 over the past 3 years; Type III, no indigenous cases reported over the past 3 years but still with risk of transmission; and Type IV, malaria-free [20]. The classification of malaria-endemic areas is presented in Figure 1 [17, 20].
Figure 1.
Stratification of malaria-endemic areas for data based on 2010 (references [5, 17]).
Several intermediate progress objectives were also set in a graduated way depending on the type of area. By 2015, (i) all Type III counties should achieve the objective of malaria elimination; (ii) at the same time, Types I and II counties, except Yunnan border counties, are expected to report zero indigenous malaria cases; (iii) the incidence of indigenous malaria cases in Type I counties located in the Yunnan border areas should be reduced to <1/10,000; (iv) it is expected that by 2017, no indigenous cases should be reported in the whole country; (v) by the year 2018, all Types I and II counties, except Yunnan border counties, must have fully achieved malaria elimination; and (vi) malaria elimination should be achieved all over the country by the year 2020.
2.2. Implementation requirements for malaria elimination
In order to achieve malaria elimination, specific requirements were assigned depending upon the type of county. The Type I counties should strengthen the management of infectious source and implement vector control measures to reduce the incidence of malaria. The Type II counties should eliminate the infectious source of malaria to interrupt local malaria transmission. The Type III counties should enhance the monitoring and disposition of the imported cases to prevent the secondary transmission. The Type IV counties should deal appropriately with imported cases. These requirements were also made flexible enough to be adjusted according to the control process and changes in the dynamics of the disease. These requirements were based on specific and standardized key measures [17].
2.2.1. Strengthening control and management of infectious sources
Timely malaria case detection. Both public and private clinics and health facilities at all levels should take blood samples from patients including clinical diagnosed malaria cases, suspected malaria cases and febrile patients without confirmed origin of infection. Blood smear for microscopic tests or auxiliary detection using Rapid Diagnosis Test (RDT) kits should be carried out with blood samples. For RDT-positive samples, blood smears must be collected and kept for verification.
Timely surveillance and response to all malaria cases [20, 21]
Strengthening malaria case reporting. Public or private clinics and health facilities at all levels have the responsibility to report malaria cases within 24 hours (1 day) after diagnosis. This is a requirement from the law on the Prevention and Control of Infectious Diseases in the People’s Republic of China (http://www.gov.cn/banshi/2005-08/01/content_19107.htm).
Case verification. Centers for Disease Control and Prevention (CDCs) at the county level are made responsible for the verification of individual cases reported through the information system and for laboratory test assessment (RDT and microscope). Case investigation and verification are required to be accomplished within 3 days after reporting.
Management of malaria foci. CDCs at the county level are responsible for investigation on identified malaria foci and further disposal within 7 days after index case reporting. A reactive case detection must be carried out by collecting blood samples from inhabitants around the index case (fever displayed over the last 2 weeks). Collected blood samples must be analyzed by microscope or RDT. Meanwhile, vector control measures (i.e., indoor residual spraying (IRS)) must be implemented, and information materials for public awareness and health education must be provided to all families in different foci.
Treatment
Full dose and whole medication3 should be given to treat malaria patients according to the national guidelines. Public or private clinics and health facilities at all levels should treat all the detected malaria patients according to the national guidelines for anti-malarial drug use, issued by the Ministry of Health. All patients must be followed up across the whole course of treatment.
Anti-relapse treatment. In non-transmission malaria season, patients diagnosed with vivax malaria during the previous year must be given anti-relapse treatment.
2.2.2. Strengthening vector control
Anti-mosquito interventions. During the malaria transmission season, it is encouraged to transform and improve the environment so as to reduce the number of breeding sites and decrease the density of mosquitoes in combination with the patriotic health movement4 and new rural village development [22]. Measures of IRS and insecticide-treated net (ITN) are required to be applied in malaria foci.
Strengthening personal protection. To prevent or minimize mosquito bites during the malaria transmission season, personal protective measures must be implemented such as repellents, mosquito-repellent incense, mosquito nets, wire mesh screening of doors and windows, etc.
2.2.3. Strengthening health education
Strengthening people awareness. Mass media such as newspapers, radio, TV, and internet posts should cover “World Malaria Day and National Malaria Day” activities and implement various ways to widely broadcast knowledge on malaria and the malaria elimination policy to improve public awareness and motivate community participation in malaria control and elimination.
Strengthening health education for primary and junior high school students. Education department should deploy and arrange the primary and junior high school health education. CDCs should strengthen the technical support to health education on malaria in these schools. Primary and junior high schools in Types I and II counties should keep malaria and malaria control awareness as a recurrent topic in regular health education courses or theme activities. They should encourage pupils to pass such awareness to their family members by the way of “child educate adult.”
Strengthening health education at the community level. In Types I and II counties, the local CDCs should organize and support malaria public awareness by the way of advertisements and regularly update posted news in hospital waiting rooms, community health service centers, rural hospitals, village clinics, and large construction sites. They should also develop awareness material in minority nations’ language.
2.2.4. Strengthening malaria control in mobile/migrant populations
Strengthening the management of malaria among travelers. The Department of Health and Exit & Entry Administration should regularly release public information about the world malaria situation and related information inside the country. Tourism departments should release such information to tourists too. The Department of Tourism and Commerce has the obligation to aid the Department of Health in providing information to people traveling to malaria-endemic areas, as well as track information on malaria patients. Mechanism for shared information should be established among different sectors. This cross sector mechanism is responsible for increasing the anti-malaria public awareness, for providing consultation services to cross-border populations, for screening individuals with fever who have been traveling to malaria-endemic areas, and for reporting the detected malaria cases.
Strengthening malaria control and prevention among expatriates. China is involved in many large construction projects in malaria epidemic areas in different countries, e.g., Ethiopia and Zambia in Africa, Myanmar and Indonesia in Southeast Asia. Some of the projects like road, railway, or dam constructions involve high malaria risk exposure. CDCs provide appropriate information and training to the personnel employed in these projects before expatriates’ deployment. The management and registration of malaria cases among expatriates are conducted locally in coordination with health agencies and CDCs. Public security departments provide assistance to investigate malaria cases among expatriates as requested by the Department of Health.
2.2.5. Improving malaria surveillance
Strengthening capacity building for malaria diagnosis. The National Institute of Parasitic Diseases, China CDC is responsible for managing national malaria diagnosis reference laboratory. Its mandate is to provide a final laboratory confirmation and identify the source of any malaria case. Reference laboratories at all levels should regularly assess the skills of test and conduct quality control to ensure operation of the laboratory network.
Malaria surveillance in the post-elimination stage. The status of malaria-free area must be maintained in counties having achieved malaria elimination, as well as in previously non-endemic provinces. This must be done through regular training of the medical personnel in malaria diagnosis and treatment. Prevention of re-establishment of malaria transmission is also required and must be conducted by intensifying the monitoring of imported cases.
3.1. Status after seven years of implementation of malaria elimination program
A total of 28,886 malaria cases were reported in Mainland China (excluding Hong Kong, Macau, and Taiwan) from 2010 to 2016 (Table 2) [9, 10, 23, 24, 25, 26]. During this period, indigenous cases, as well as the number of areas with local transmission, were substantially reduced. There were 40 indigenous cases reported from 10 counties in 2015, a decrease of 99.06% from 2010. By 2015, all Type III counties had achieved malaria elimination goals (no occurrence of indigenous cases for at least 3 consecutive years). Except for border counties in Yunnan, 96.43% (54/56) of the Type I counties reported no indigenous case over the same period. The malaria incidence in 19 Type I counties in Yunnan border area was lower than 10/100,000. All positive cases were reported through the China Information System for Disease Control and Prevention (CISDCP). The increase in incidence and number of detected cases after 6 years of implementation of the malaria elimination program was linked to the large number of imported cases, while the number of indigenous cases was reduced by 99.93% between 2010 and 2016 (Table 2) [8, 27, 28, 29, 30]. The number of provinces with imported cases increased from 22 in 2010 to 30 (all the provinces in Mainland China except Tibet) in 2015. A total of 3318 imported cases were reported in 2016 (Table 2). The top 5 countries of origin of the imported cases were Myanmar (15.9%), Angola (12.5%), Nigeria (7.7%), Equatorial Guinea (7.5%), and Cameroon (7.1%). In response to the increasing risk from imported cases, joint coordination and transfer of information were established among different agencies, in particular between China CDC and port quarantines. The latter are responsible for frontline screening and detection providing timely reports of positive cases. Clinics and hospitals are in charge of case treatment, while CDCs must follow up all the reported cases and carry out the individual case investigation. A successful example of such organization is given by the Shanglin County, Guangxi [31], for reporting 1,052 imported malaria cases in 2013, all of which were successfully treated and no death cases occurred. Furthermore, although Anopheles mosquitoes were present [14], no secondary transmission occurred.
Malaria-attributable morbidity in the People’s Republic of China during 2010–2016°.
The number of malaria cases reported in 2017 will be published by the end of 2018.
NA indicates that data were not available in the annual reporting system.
Before 2013, the data recorded in the annual reporting system did not separate P. malariae and P. ovale.
Along the border between China and countries of the Greater Mekong Subregion (GMS) (Myanmar, Lao PDR, and Vietnam), 3 frontline barriers were established jointly by CDCs and port quarantines [32]. These 3 barriers consisted of (i) a strengthened health system in all 25 border counties with a capacity to immediate and comprehensive response to each malaria case (first line), (ii) establishment of 68 malaria service points at the border to provide consultation and screening to the migrant/mobile population (MMP) (second line), and (iii) a coordination process for response to malaria along the international borders between China, Myanmar, Lao PDR, and Vietnam covering 42 border counties (20 in Yunnan and 22 in the 3 other countries).
The main risks clearly identified after implementation of the national malaria elimination program were re-introduction through imported cases and the associated secondary transmission by local malaria vectors. Sustainable vector control is therefore essential. With the support from the national malaria surveillance system and national malaria diagnosis reference laboratory network, all the confirmed malaria cases were examined, including a total number of 2,215 foci investigated within 7 days after case detection and verification (Table 3). Long-lasting insecticidal net (LLIN) or ITN was delivered to the communities with high malaria incidence and presence of highly efficient malaria vectors, such as Anopheles dirus s.l. or Anopheles minimus s.l. [14]. IRS was carried out in active malaria foci (the definition of active foci is given in Ref. [19, 33]). In 2015, a total number of 29,611 LLIN/ITN were delivered, and 1,697,188 persons were protected by IRS in response to malaria foci (Table 4). Another key element in the protection of people against imported malaria was the training and education of the personnel. Annual joint health training workshops were carried out by the Departments of Health, Education, and Inspection and Quarantine on the National Malaria Day (April 26th) since 2008. Altogether, 74.9 million educational documents were delivered during workshops from 2010 to 2015 (Table 5). To these, one must add all posters and flyers delivered through port quarantines. Capacity building for health professional personnel corresponded to 464,500 working days in CDCs; 848,764 working days for clinical doctors; and 186,368 working days for microscopists during 2010–2015 (Table 5). With respect to port quarantines, 16,141 working days of training were accomplished with a malaria awareness rate of 100%.
Province
Cases reported within 24 h
Case investigation within 3 days
Number of foci investigated and disposed within 7 days
1-3-7 model is referring to case reported within 1 day (24 hours), case verification and investigation within 3 days, and foci investigation and disposal within 7 days. This is summarized as work model for malaria surveillance and response for malaria elimination program [20, 21].
Progress indicators of vector control measures in 2015.
Vector control measures mainly implemented in malaria foci for targeting population at risk.
Province
Number of trained people (person/time)
Number of delivered health education materials
Malaria health workers
Clinical doctors
Microscopists
Beijing
208
0
176
185,000
Tianjin
240
300
300
25,700
Hebei
41,499
95,926
10,652
3,064,121
Shanxi
596
0
871
57,000
Inner Mongolia
204
408
204
3200
Liaoning
7554
88,609
5835
143,600
Jilin
226
0
226
4000
Heilongjiang
0
0
0
0
Shanghai
21,516
48,584
9377
1,246,268
Jiangsu
26,415
23,963
16,468
7,365,562
Zhejiang
11,447
19,304
8749
1,676,164
Anhui
59,229
42,417
18,671
14,323,973
Fujian
7653
8777
3095
556,489
Jiangxi
12,696
24,829
9272
1,621,293
Shandong
34,624
56,382
15,494
7,040,504
Henan
62,005
183,085
19,486
7,968,270
Hubei
27,199
38,291
10,062
4,078,954
Hunan
22,018
46,761
11,666
4,722,609
Guangdong
737
375
1008
429,401
Guangxi
23,682
57,461
10,914
4,505,439
Hainan
10,838
5288
2607
2,058,430
Chongqing
1027
0
235
0
Sichuan
1900
0
825
372,200
Guizhou
21,643
28,120
8827
3,342,021
Yunnan
28,962
35,103
7479
4,200,909
Tibet
—
—
—
—
Shaanxi
21,951
34,313
10,970
3,615,648
Gansu
12,851
9136
2178
1,631,944
Qinghai
—
—
—
—
Ningxia
469
0
144
0
Xinjiang
5111
1332
577
670,755
Total
464,500
848,764
186,368
74,909,454
Table 5.
Progress indicators of health education and capacity building during 2010–2015.
Note: “-” denotes data not available.
A key issue in successful implementation of a program relies on the governmental commitment and support for sustained allocation of resources. The government at all levels has adopted malaria elimination as a component of the socioeconomic strategy. A national action plan for malaria elimination was issued jointly by 13 ministries in 2010 with clear goals and strategy, followed by a sustainable budget plan to ensure the financial support for malaria elimination. As a key player in malaria elimination in the central government, the National Health Commission (NHC, previously known as the Ministry of Health before 2011 and National Health and Family Planning Commission during 2011–2018) has established a multidisciplinary technical committee comprising malaria experts, i.e., epidemiologists, entomologists, clinical doctors, parasitologists, program managers, etc. With the support of this committee, NHC has issued a series of guidelines and standards adapting and updating the WHO guidelines [2, 19, 33, 34], such as technical guidelines for malaria elimination, malaria treatment and anti-malarial drug use, standards for malaria control and elimination, and malaria diagnosis, to cite a few [18].
3.2. Successful implementation
A working model, named 1-3-7, for malaria surveillance and response was implemented as a national malaria program. The definition of “1-3-7” is as follow:
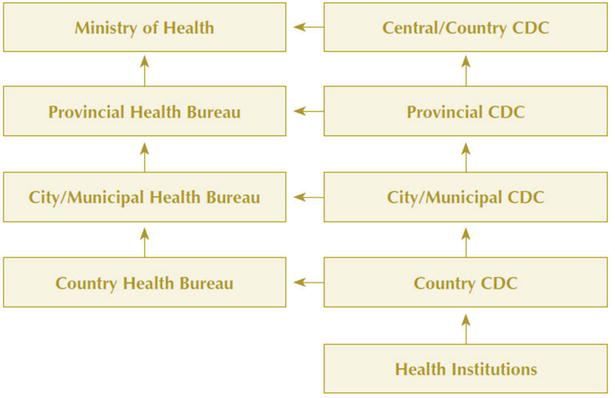
“1,” within 1 day (24 hours): all malaria cases must be reported to the Chinese Information System for Disease Control and Prevention (CISDCP), an internet-based reporting system. The case information will be notified through a four-level system “county→ prefecture→ province→ national.” The response at different levels is implemented according to national guidelines. Malaria is classified as a category B notifiable infectious disease, and case reporting through CISDCP has been implemented since 2004 [35]. All private and public registered clinics and hospitals must report malaria cases through CISDCP after diagnosis. CDCs are the key operators of CISDCP (Figure 2). This ensures that malaria case information is timely transmitted from bottom to top.
“3,” within 3 days: all the reported malaria cases should be confirmed and visited by CDCs’ staffs at the county level to verify the infectious origin of the cases (whether imported or locally acquired). Meanwhile, blood samples of patients are taken and sent to the reference laboratory for further verification.
“7,” within 7 days: the outbreak focus should be investigated, and vector control and health promotion measures must be implemented. Vector control measures need to be conducted in active foci only, which are considered to have potential risk of onward transmission. The scope of investigation is the household of the reported patient and neighboring households. However, it can be expanded, if necessary.
Figure 2.
Vertical reporting structure of the China information system for disease control and prevention (CISDCP) (CDC, Centers for Disease Control and Prevention).
Following the implementation of this 1-3-7 model, local malaria transmission was interrupted effectively in most parts of China, which accelerated the malaria elimination process [20, 21, 36]. Based on this success, the 1-3-7 model was recommended by WHO as an example for malaria surveillance model at elimination stage, in “Strategy for malaria elimination in the Greater Mekong Subregion: 2015-2030” and “Malaria surveillance, monitoring & evaluation: a reference manual” [37, 38].
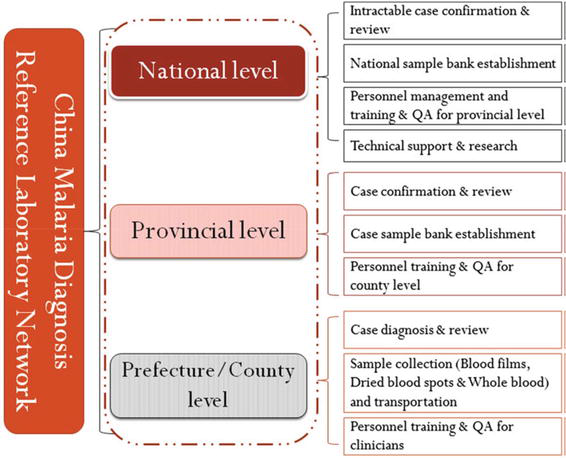
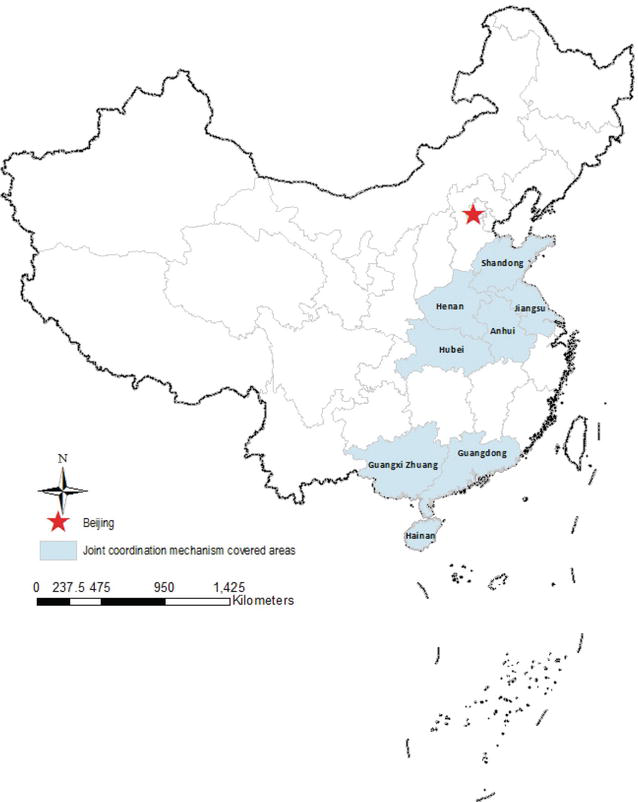
However, the 1-3-7 strategy is not sufficient to successfully achieve malaria elimination. Other aspects must be considered. The first aspect to consider is the establishment of a network of malaria surveillance and diagnosis reference laboratories. After the launch of the malaria elimination program in 2010, and following the suggestions from the WHO guidelines [2, 19, 33, 34], a network for malaria diagnosis reference labs was gradually established [39]. By 2015, 23 provinces were enrolled into the National Reference Laboratory Network (NRLN). Laboratories at all levels worked together to ensure the quality of malaria diagnosis all over the country in a bottom-up approach (Figure 3) [39]. Another key aspect to consider is the involvement of communities. The community level is essential for a successful implementation. In addition to cross sector coordination, information was shared with different subnational divisions and in particular the community level. This is especially important when managing malaria cases among mobile/migrant populations. Five provinces in Central China, i.e., Jiangsu, Shandong, Henan, Anhui, and Hubei, and 3 provinces in Southern China, i.e., Guangdong, Guangxi, and Hainan, coordinated their actions at all levels (Figure 4). This joint coordination efficiently contributed to control malaria outbreaks and reduce malaria incidence [40, 41]. The last aspect to be considered is international collaboration. Malaria elimination cannot be achieved through the efforts of few countries only. It must be a general and coordinated international effort. In this respect, China has received support from international agencies such as WHO and Global Fund to Fight AIDS, Tuberculosis and Malaria (GFATM) to conduct this international collaboration [42]. At the same time, China developed international collaborations with African and GMS countries to implement a coordinated strategy for controlling and eliminating malaria [43, 44], and Chinese students are being trained in Europe on molecular approaches applied on Anopheles mosquitoes [13, 14, 15]. These international collaborations on malaria and vector control toward elimination provided strong support to reduce malaria incidence in China and will be the basis for sustaining malaria elimination efforts.
Figure 3.
Structure of the National Reference Laboratory Network (QA, quality assurance).
Figure 4.
Cross province coordination mechanism for malaria control based on national mechanisms established since the 1950s–1970s. At that time, few population movements were occurring in the Yunnan Province.
Although the malaria elimination program has made significant progress in China, there are still challenges. The main challenge is to accomplish malaria elimination along border areas. China is sharing 4060 km long international borders with GMS countries. These borders are devoid of natural barriers and porous, permitting population movement and facilitating cross border malaria transmission. The China-Myanmar border is particularly difficult to access for healthcare services due to ongoing armed conflict on the Myanmar side of the border resulting in proliferation of disease vectors and uninterrupted disease transmission [13, 15, 32, 45, 46, 47, 48]. A related challenge is the prevention of re-introduction and re-establishment of malaria considered as a real threat to malaria elimination [2, 33, 34, 37]. Surveillance is highly recommended as a key intervention in the post-malaria elimination stage. However, decisive and rapid response to imported malaria is vital to prevent re-introduction and sustain malaria elimination [11, 27, 29, 49, 50, 51, 52, 53]. A shift from community to hospitals at the county and higher level for primary diagnosis was also recorded [8, 27], indicative of a more active role of the main city airports as ports of entry. In addition, owing to the sharp decrease of indigenous cases, it becomes difficult to maintain the capacity of intervention and proper training at the local level. Novel and innovative capacity building and training modules must thus be developed for both clinicians and CDC staffs.
The main objective in China with respect to malaria will be focused on how to sustain malaria elimination and prevent transmission re-establishment in accordance with the WHO’s newly updated guidelines [33]. This requires a specific and sustainable investment even at post-elimination stage. Malaria is on the list of the “Health China 2030” blueprint issued by the State Council of China in 2016. This will ensure the required sustainable investment. Following this blueprint, a series of technical guidelines for malaria surveillance and response at post-elimination stage, as well as protocols for preventing malaria transmission re-establishment, are under development for short release. Meanwhile, mechanisms for maintaining anti-malaria capacity in health system are implemented. A National Technical Competition for Parasitic Disease Diagnosis and Test is organized annually for health workers from clinical agencies and CDCs [54]. This competition is an efficient way to maintain awareness and efficiency in malaria detection within the health system and prevent erosion of capacity along with malaria elimination. However, malaria elimination is primarily an international endeavor. Broad engagement and sustained investments are needed with support from multiple international partners [55, 56, 57]. In 2013, Chinese President Xi Jinping proposed the “One Belt and One Road Initiatives” to the world for international cooperation and development. Cooperation in health is one of the key components as it relates to the mutual benefits. China has already been actively involved in global health governance [58], but a higher level of involvement is now expected, and the Chinese experience in malaria elimination will definitely be put at use within the “One Belt and One Road Initiative” [59]. Several platforms are currently under development, such as the Malaria Elimination Network in Lancang-Mekong Region (MENLMR) and the China-Africa Cooperation Program. Both GMS and sub-Saharan Africa are strongly affected by malaria, including drug resistance [60, 61, 62], high disease burden [1], and low level of resources [1, 3, 34]. They are thus primary targets for focused interventions enabling malaria elimination. Furthermore, these countries are experiencing innumerable challenges to achieve their planned malaria elimination program and in dire need of international support to bridge the funding gap [1, 2, 3, 37]. Although China has applied a successful model and did significant progress on malaria elimination, the Chinese model and experience cannot directly be implemented in these countries. Evaluation and field tests are needed as preliminary steps for operational feasibility. Pilot areas have been identified, and demonstrative projects have been therefore launched jointly by China and the targeted countries to assess the level of feasibility. These preliminary projects will provide evidence-based suggestions to develop a suitable strategy and model for each country to realize the ultimate goal of malaria elimination.
China has made substantial progress on malaria elimination and is on the way to achieve the elimination goal on time by 2020. The lessons drawn based on experiences in China will make a good reference for the countries aiming at malaria elimination. Challenges identified in the malaria elimination process in China might help other countries formulating appropriate strategies in time and place. International collaboration is strongly advocated to achieve the global issue to eliminate the most important infectious disease of the current times.
All the staffs in 31 provincial CDCs who have provided support to the data collection are acknowledged. This study was supported by TDR training grant (B40084).
China Information System for Disease Control and Prevention
DDT
Dichlorodiphenyltrichloroethane
E-2020
In 2016, the WHO identified 21 countries with the potential to eliminate malaria by the year 2020. These countries were known as “E-2020 countries
GFATM
Global Fund to Fight AIDS, Tuberculosis and Malaria
GMS
Greater Mekong Subregion
IRS
Indoor residual spraying
ITN
Insecticide-treated net
LLIN
Long-lasting insecticidal net
MENLMR
Malaria Elimination Network in Lancang-Mekong Region
MDGs
UN Millennium Development Goals
MMP
Mobile and migrant population
NHC
National Health Commission
NRLN
National Reference Laboratory Network
QA
Quality assurance
RDT
Rapid diagnosis test
TDR
Special Programme for Research and Training in Tropical Diseases
WHO
World Health Organization
References
1.WHO. World Malaria Report. Geneva, Switzerland: World Health Organization; 2017. p. 196
2.WHO. Global Technical Strategy for Malaria 2016-2030. Geneva, Switzerland: World Health Organization; 2015
3.Alonso P, Noor AM. The global fight against malaria is at crossroads. Lancet. 2017;390(10112):2532
4.Zhou XN, Xia ZG, Wang RB, Qian YJ, Zhou SS, Utzinger J, Tanner M, Kramer R, Yang WZ. Feasibility and roadmap analysis for malaria elimination in China. Advances in Parasitology. 2014;86:21-46
5.Yin JH, Zhou SS, Xia ZG, Wang RB, Qian YJ, Yang WZ, Zhou XN. Historical patterns of malaria transmission in China. Advances in Parasitology. 2014;86:1-19
6.Hu T, Liu YB, Zhang SS, Xia ZG, Zhou SS, Yan J, Cao J, Feng ZC. Shrinking the malaria map in China: Measuring the progress of the National Malaria Elimination Programme. Infectious Diseases of Poverty. 2016;5(1):52
7.WHO. World Malaria Report 2016. Geneva, Switzerland; 2016. p. 186
8.Feng J, Zhang L, Zhang SS, Xia ZG, Zhou SS. Malaria epidemiological characteristics in China, 2005-2015. China Tropical Medicine. 2017;17(4):325-335
9.Zhang L, Feng J, Zhang SS, Xia ZG, Zhou SS. Malaria situation in the People's Republic of China in 2015. Chinese Journal of Parasitology and Parasitic Diseases. 2016;34(6):477-481
10.Zhang L, Zhou SS, Feng J, Fang W, Xia ZG. Malaria situation in the People' s republic of China in 2014. Chinese Journal of Parasitology & Parasitic Diseases. 2015;33(5):319-326
11.Feng J, Xiao H, Zhang L, Yan H, Feng X, Fang W, Xia Z. The Plasmodium vivax in China: Decreased in local cases but increased imported cases from Southeast Asia and Africa. Scientific Reports. 2015;5:8847
12.Feng J, Xiao H, Xia Z, Zhang L, Xiao N. Analysis of malaria epidemiological characteristics in the People's Republic of China, 2004-2013. The American Journal of Tropical Medicine and Hygiene. 2015;93(2):293-299
13.Zhang SS, Zhou SS, Zhou ZB, Wang XZ, Jiang WK, Shi WQ, Yang YH, Yin SQ, Li XS, Wang JZ, Li SG, Zhang Y, Zhou XN. Investigation on population density and bionomics of Anopheles minimus in China-Myanmar border areas Yunnan province, P.R. China. Chinese Journal of Vector Biology and Control. 2017;28(3):216-219,254
14.Zhang SS, Guo SH, Feng XY, Afelt A, Frutos R, Zhou SS, Manguin S. Anopheles vectors in mainland China while approaching malaria elimination. Trends in Parasitology. 2017;33(11):889-900
15.Chen T, Zhang SS, Zhou SS, Wang X, Luo C, Zeng X, Guo X, Lin Z, Tu H, Sun X, Zhou H. Receptivity to malaria in the China-Myanmar border in Yingjiang County, Yunnan Province, China. Malaria Journal. 2017;16(1):478
16.Feng X, Zhang S, Huang F, Zhang L, Feng J, Xia Z, Zhou H, Hu W, Zhou S. Biology, bionomics and molecular biology of Anopheles sinensis Wiedemann 1828 (Diptera: Culicidae), main malaria vector in China. Frontiers in Microbiology. 2017;8:1473
17.China Ministry of Health. Action Plan of China Malaria Elimination (2010-2020). Beijing: Ministry of Health and other 12 Ministries in P.R. China; 2010
18.Tang LH, Gao Q. Malaria Control and Elimination in China. 1st ed. Shanghai: Shanghai Scientific & Technical Publishers; 2013. p. 197
19.WHO. Malaria Elimination. A Field Manual for Low and Moderate Endemic Countries. Geneva, Switzerland: World Health Organization; 2007
20.Zhou SS, Zhang SS, Zhang L, Rietveld AE, Ramsay AR, Zachariah R, Bissell K, Van den Bergh R, Xia ZG, Zhou XN, Cibulskis RE. China's 1-3-7 surveillance and response strategy for malaria elimination: Is case reporting, investigation and foci response happening according to plan? Infectious Diseases of Poverty. 2015;4:55
21.Cao J, Sturrock HJ, Cotter C, Zhou S, Zhou H, Liu Y, Tang L, Gosling RD, Feachem RG, Gao Q. Communicating and monitoring surveillance and response activities for malaria elimination: China's “1-3-7” strategy. PLoS Medicine. 2014;11(5):e1001642
22.Bu L. Anti-Malaria Campaigns and the Socialist Reconstruction of China. 1950-1980; 2014
23.Zhang L, Feng J, Xia ZG. Malaria situation in the People's Republic of China in 2013. Chinese Journal of Parasitology and Parasitic Diseases. 2014;32(6):407-413
24.Xia ZG, Feng J, Zhou SS. Malaria situation in the People's Republic of China in 2012. Chinese Journal of Parasitology and Parasitic Diseases. 2013;31(6):413-418
25.Xia ZG, Yang MN, Zhou SS. Malaria situation in the People's Republic of China in 2011. Chinese Journal of Parasitology and Parasitic Diseases. 2012;30(6):419-422
26.Zhou SS, Wang Y, Li Y. Malaria situation in the People's Republic of China in 2010. Chinese Journal of Parasitology and Parasitic Diseases. 2011;29(6):401-403
27.Zhou S, Li Z, Cotter C, Zheng C, Zhang Q, Li H, Zhou S, Zhou X, Yu H, Yang W. Trends of imported malaria in China 2010-2014: Analysis of surveillance data. Malaria Journal. 2016;15:39
28.Li Z, Zhang Q, Zheng C, Zhou S, Sun J, Zhang Z, Geng Q, Zhang H, Wang L, Lai S, Hu W, Clements AC, Zhou XN, Yang W. Epidemiologic features of overseas imported malaria in the People's Republic of China. Malaria Journal. 2016;15:141
29.Wang D, Li S, Cheng Z, Xiao N, Cotter C, Hwang J, Li X, Yin S, Wang J, Bai L, Zheng Z, Wang S. Transmission risk from imported Plasmodium vivax malaria in the China-Myanmar border region. Emerging Infectious Diseases. 2015;21(10):1861-1864
30.Yin JH, Yang MN, Zhou SS, Wang Y, Feng J, Xia ZG. Changing malaria transmission and implications in China towards National Malaria Elimination Programme between 2010 and 2012. PLoS One. 2013;8(9):e74228
31.Li Z, Yang Y, Xiao N, Zhou S, Lin K, Wang D, Zhang Q, Jiang W, Li M, Feng X, Yu J, Ren X, Lai S, Sun J, Fang Z, Hu W, Clements AC, Zhou X, Yu H, Yang W. Malaria imported from Ghana by returning gold miners, China, 2013. Emerging Infectious Diseases. 2015;21(5):864-867
32.Yang HL, Xiao N, Yang YM, Xu JW. Challenges, opportunities and strategies of malaria elimination along China-Myanmar and China- Laos border. China Tropical Medicine. 2017;17(4):321-335
33.WHO. A Framework for Malaria Elimination. Geneva, Switzerland: World Health Organization; 2017
34.WHO. Eliminating Malaria. Geneva, Switzerland: World Health Organization; 2016
35.Wang L, Wang Y, Jin S, Wu Z, Chin DP, Koplan JP, Wilson ME. Emergence and control of infectious diseases in China. Lancet. 2008;372(9649):1598
36.Lu G, Liu Y, Beiersmann C, Feng Y, Cao J, Muller O. Challenges in and lessons learned during the implementation of the 1-3-7 malaria surveillance and response strategy in China: A qualitative study. Infectious Diseases of Poverty. 2016;5(1):94
37.WHO. Strategy for Malaria Elimination in the Greater Mekong Subregion: 2015-2030. Geneva, Switzerland: World Health Organization; 2015
38.WHO. Malaria surveillance, Monitoring & Evaluation: A Reference Manual. Geneva, Switzerland: World Health Organization; 2018
39.Yin JH, Yan H, Huang F, Li M, Xiao HH, Zhou SS, Xia ZG. Establishing a China malaria diagnosis reference laboratory network for malaria elimination. Malaria Journal. 2015;14:40
40.Shang LY, Gao Q, Liu X, Shen YZ, Huang GQ. Evaluation on the effect of cooperative malaria control in 5 provinces of Central China in 30 years. Journal of Pathogen Biology. 2006;1(1):51-53
41.Zhang HW, Liu Y, Zhang SS, Xu BL, Li WD, Tang JH, Zhou SS, Huang F. Preparation of malaria resurgence in China: Case study of vivax malaria re-emergence and outbreak in Huang-Huai plain in 2006. Advances in Parasitology. 2014;86:205-230
42.Wang RB, Zhang QF, Zheng B, Xia ZG, Zhou SS, Tang LH, Gao Q, Wang LY, Wang RR. Transition from control to elimination: Impact of the 10-year global fund project on malaria control and elimination in China. Advances in Parasitology. 2014;86:289-318
43.Xia ZG, Zhang L, Feng J, Li M, Feng XY, Tang LH, Wang SQ, Yang HL, Gao Q, Kramer R, Ernest T, Yap P, Zhou XN. Lessons from malaria control to elimination: Case study in Hainan and Yunnan provinces. Advances in Parasitology. 2014;86:47-79
44.Xia ZG, Wang RB, Wang DQ, Feng J, Zheng Q, Deng CS, Abdulla S, Guan YY, Ding W, Yao JW, Qian YJ, Bosman A, Newman RD, Ernest T, O'Leary M, Xiao N. China-Africa cooperation initiatives in malaria control and elimination. Advances in Parasitology. 2014;86:319-337
45.Zhang Q, Sun J, Zhang Z, Geng Q, Lai S, Hu W, Clements AC, Li Z. Risk assessment of malaria in land border regions of China in the context of malaria elimination. Malaria Journal. 2016;15(1):546
46.Wang D, Cotter C, Sun X, Bennett A, Gosling RD, Xiao N. Adapting the local response for malaria elimination through evaluation of the 1-3-7 system performance in the China-Myanmar border region. Malaria Journal. 2017;16(1):54
47.Shi B, Zheng J, Qiu H, Yang GJ, Xia S, Zhou XN. Risk assessment of malaria transmission at the border area of China and Myanmar. Infectious Diseases of Poverty. 2017;6(1):108
48.Xu JW, Liu H. The relationship of malaria between Chinese side and Myanmar's five special regions along China-Myanmar border: A linear regression analysis. Malaria Journal. 2016;15(1):368
49.Sriwichai P, Karl S, Samung Y, Kiattibutr K, Sirichaisinthop J, Mueller I, Cui L, Sattabongkot J. Imported Plasmodium falciparum and locally transmitted Plasmodium vivax: Cross-border malaria transmission scenario in northwestern Thailand. Malaria Journal. 2017;16(1):258
50.Xu C, Wei QK, Li J, Xiao T, Yin K, Zhao CL, Wang YB, Kong XL, Zhao GH, Sun H, Liu X, Huang BC. Characteristics of imported malaria and species of Plasmodium involved in Shandong Province, China (2012-2014). The Korean Journal of Parasitology. 2016;54(4):407-414
51.Cao Y, Wang W, Liu Y, Cotter C, Zhou H, Zhu G, Tang J, Tang F, Lu F, Xu S, Gu Y, Zhang C, Li J, Cao J. The increasing importance of Plasmodium ovale and Plasmodium malariae in a malaria elimination setting: An observational study of imported cases in Jiangsu Pro-vince, China, 2011-2014. Malaria Journal. 2016;15:459
52.Feng J, Yan H, Feng XY, Zhang L, Li M, Xia ZG, Xiao N. Imported malaria in China, 2012. Emerging Infectious Diseases. 2014;20(10):1778-1780
53.Feng J, Xia ZG, Vong S, Yang WZ, Zhou SS, Xiao N. Preparedness for malaria resurgence in China: Case study on imported cases in 2000-2012. Advances in Parasitology. 2014;86:231-265
54.Zhang SS, Xia ZG, Yin JH, Yan H, Zhou SS, Li SZ, Zheng X, Huang F, Li M, Chen HT, Wang Q, Zhang L, Liu W, Xiao N, Zhou XN. Analysis report of National Technical Competition for diagnosis of parasitic diseases in 2012: I. Capability analysis of Plasmodium detection. Chinese Journal of Parasitology and Parasitic Diseases. 2013;31(2):131-134
55.Rabinovich RN, Drakeley C, Djimde AA, Hall BF, Hay SI, Hemingway J, Kaslow DC, Noor A, Okumu F, Steketee R, Tanner M, Wells TNC, Whittaker MA, Winzeler EA, Wirth DF, Whitfield K, Alonso PL. malERA: An updated research agenda for malaria elimination and eradication. PLoS Medicine. 2017;14(11):e1002456
56.The malERA Refresh Consultative Panel on Health Systems and Policy Research. malERA: An updated research agenda for health systems and policy research in malaria elimination and eradication. PLoS Medicine. 2017;14(11):e1002454
57.Cibulskis RE, Alonso P, Aponte J, Aregawi M, Barrette A, Bergeron L, Fergus CA, Knox T, Lynch M, Patouillard E, Schwarte S, Stewart S, Williams R. Malaria: Global progress 2000-2015 and future challenges. Infectious Diseases of Poverty. 2016;5(1):61
58.Liu P, Guo Y, Qian X, Tang S, Li Z, Chen L. China's distinctive engagement in global health. Lancet. 2014;384(9945):793-804
59.Tang K, Li Z, Li W, Chen L. China's silk road and global health. Lancet. 2017;390(10112):2595-2601
60.Sinha S, Medhi B, Sehgal R. Challenges of drug-resistant malaria. Parasite. 2014;21:61
61.Ashley EA, Dhorda M, Fairhurst RM, Amaratunga C, Lim P, Suon S, Sreng S, Anderson JM, Mao S, Sam B, Sopha C, Chuor CM, Nguon C, Sovannaroth S, Pukrittayakamee S, Jittamala P, Chotivanich K, Chutasmit K, Suchatsoonthorn C, Runcharoen R, Hien TT, Thuy-Nhien NT, Thanh NV, Phu NH, Htut Y, Han KT, Aye KH, Mokuolu OA, Olaosebikan RR, Folaranmi OO, Mayxay M, Khanthavong M, Hongvanthong B, Newton PN, Onyamboko MA, Fanello CI, Tshefu AK, Mishra N, Valecha N, Phyo AP, Nosten F, Yi P, Tripura R, Borrmann S, Bashraheil M, Peshu J, Faiz MA, Ghose A, Hossain MA, Samad R, Rahman MR, Hasan MM, Islam A, Miotto O, Amato R, MacInnis B, Stalker J, Kwiatkowski DP, Bozdech Z, Jeeyapant A, Cheah PY, Sakulthaew T, Chalk J, Intharabut B, Silamut K, Lee SJ, Vihokhern B, Kunasol C, Imwong M, Tarning J, Taylor WJ, Yeung S, Woodrow CJ, Flegg JA, Das D, Smith J, Venkatesan M, Plowe CV, Stepniewska K, Guerin PJ, Dondorp AM, Day NP, White NJ. Tracking resistance to artemisinin C. Spread of artemisinin resistance in Plasmodium falciparum malaria. The New England Journal of Medicine. 2014;371(5):411-423
62.Na-Bangchang K, Karbwang J. Emerging artemisinin resistance in the border areas of Thailand. Expert Review of Clinical Pharmacology. 2013;6(3):307-322
Notes
Botswana, Cabo Verde, South Africa, Swaziland, Costa Rica, Ecuador, El Salvador, Mexico, Saudi Arabia, Timor-Leste, Malaysia.
Botswana, South Africa, Swaziland, Ecuador, Saudi Arabia.
Whole medication refers to the 8-day treatment for vivax malaria with primaquine (total dose 180 mg over 8 days) and chloroquine (total dose 1200 mg over 3 days) as first-line drugs. Artemisinin combination therapy (ACT) was used as first-line treatment to treat uncomplicated falciparum malaria.
The patriotic health movement is referring to a community-based health movement focusing on cleaning, pest control, environment reforming, and other health-related activities, with the aim of preventing infectious diseases.
Written By
Shaosen Zhang, Li Zhang, Jun Feng, Jianhai Yin, Xinyu Feng, Zhigui
Xia, Roger Frutos, Sylvie Manguin and Shuisen Zhou
Submitted: January 15th, 2018Reviewed: April 16th, 2018Published: July 18th, 2018