


Abstract
Complex systems at different levels (states, organisations, individuals) undergo phase transitions when faced with a sudden shock. The phase transitions are unpredictable and can lead to unstable states and also introduce a source of fundamental uncertainty about the future. In the face of this type of fundamental uncertainty, we know from pioneering work on population health that social determinants (e.g. education, employment, housing, etc.) will have a substantial influence on the ability of individuals and society to be resilient and recover from these shocks. This chapter will start with an overview of complex systems, phase transitions and the nature of fundamental uncertainty. These concepts will then be discussed in light of the COVID-19 pandemic. The importance of social determinants in promoting both mental and physical health, and thus resilience at individual and population levels, will be described and the chapter will finish with an exploration of historical and contemporary examples of means that can be used to support individual and collective resilience in the face of fundamental uncertainty.
Keywords
- Population health
- social determinants of health
- phase transitions
- complex systems
- resilience
1. Introduction
The COVID-19 pandemic has been devastating and it has affected all aspects of society around the world. Three areas that have been particularly negatively affected are the economy, health and education.
In 2020, we saw a 5.2% contraction in global GDP and estimates suggest that the global unemployment rate could increase from 4.9–5.6% [1, 2, 3]. Per capita income has also contracted globally and in the largest proportion of countries since 1870 [1]. In aggregate, the negative impacts on the economy could lead to up to 300 million people internationally falling below the poverty line and between 70 and 100 million people may have fallen into extreme poverty in 2020 [4, 5]. And all of this despite the various efforts by governments to shore up economies leading global debt to increase by $24 trillion over the past year – a level of debt much higher than seen with the 2008 global financial collapse [6, 7].
Overlaid onto the negative impacts on the economy are affects the pandemic has had on health beyond COVID-19 infections. Disruptions to global trade saw global food prices increase by ~20% between January 2020 and January 2021, which, combined with reduced incomes, means that households will have to decrease the quantity and quality of food they are consuming [8]. Indeed, country surveys across countries globally indicated up to 40% of households were running out of food or reducing their consumption with an average of 50% of households in the poorest countries confirming that someone was skipping at least one meal [4, 8]. Across 79 countries, the total number of acutely food insecure people was expected to increase to 272 million by the end of 2020 [8].
Mental health has also been impacted by the pandemic and its associated lockdown measures. Individuals with existing mental illness have experienced a detrimental impact on their mental health with some countries seeing a two-fold increase in the number of adults experiencing some form of depression [9, 10]. The increases in unemployment, increased financial difficulties, social isolation, uncertainty about the future and disruption to clinical services could contribute to increased alcohol intake as well as an increase in suicides [3, 11, 12, 13].
The pandemic has also been difficult for children and youth. The lockdown measures associated with the COVID-19 pandemic represents the largest disruption to education systems in history and has affected over 1.6 billion learners in over 190 countries, which represents 94% of the world’s student population [14, 15, 16, 17]. The shift to remote learning was helpful for some but many students globally, especially those of poorer households, lack access to internet and digital technologies and will fall further behind. It is estimated that we will see a 25% increase in the proportion of children below minimum education proficiency [15, 18]. School closures also affects the provision of essential services and benefits (e.g. access to nutritious food, supporting the ability of parents to work, etc.) to families in need [16, 17].
The short-, medium- and long-term impacts we are seeing with the COVID-19 pandemic, and which we will continue to see in its aftermath, will have unpredictable impacts because of the complexity of the systems (states, organisations, individuals) being impacted. When faced with a sudden shock like the COVID-19 pandemic, or other crises like the 2008 global financial collapse, complex systems undergo unpredictable transitions that could have significant impacts on the ability of individuals and society to be resilient and recover from these shocks. The fundamental uncertainty about if, when and how these transitions occur for complex systems makes it difficult to know exactly what will happen and/or what to do to reduce potential negative impacts.
This chapter will start with an overview of complex systems, phase transitions and the nature of fundamental uncertainty, which will then be discussed in the context of the COVID-19 pandemic. The importance of social determinants of health in promoting both mental and physical health, and thus resilience at individual and population levels, will be described and the chapter will finish with an exploration of historical and contemporary examples of means that can be used to support individual and collective resilience in the face of the fundamental uncertainty of the world post-COVID-19.
2. Phase transitions of complex systems: contextualising fundamental uncertainty
2.1 Complex systems
Systems are present everywhere. A simple definition definition of systems is a set of interconnected elements that produce their own patterns of behaviour. The system will have its internal drivers and will also be influenced by external factors – how a system responds to external factors through its internal mechanisms is an inherent characteristic of a given system [19]. Starting with this basic definition, one quickly realises that the world can be seen through the lens of systems – whether that be at an organismal, organisational, societal, state and/or global level. A key consideration for any system, at whatever level, is its complexity because how a system behaves is not always simple, or even possible to predict.
The complexity of a system is related to the number of elements it has and their connections and feedback loops. These considerations reveal that complex systems:
Nonlinearity, interconnectedness and emergence are three characteristics that make it difficult to predict exactly how a complex system will behave. The non-linear behaviour and interconnectedness of a complex system’s elements means that it is subject to irreversibility - external factors or inputs into a complex system can be removed but that does not mean that the complex system can return to its original state – as well as the power law, which means that an effect on the complex system will lead to an impact that is much greater than would normally be expected. These two factors combine to support the emergent behaviour of a complex system which sees large impacts resulting from simple, small-scale changes – or to put it another way, the sum is greater than the parts. The implications of these features of complex systems means that if a complex system is subject to a sudden external shock, the changes to the system are not predictable, reversible and, in many cases, manageable [21].
A classic example demonstrating these three factors in action is a traffic jam. Over a large range of car density on a highway, car speed is only slightly affected but there will be a threshold/tipping point, characteristic of a given highway, beyond which a small increase in car density can lead to a disproportionate decrease in traffic flow resulting in a traffic jam. Another example is the transition of water from solid to liquid or liquid to gas – there is a critical threshold of pressure and temperature at which water will freeze, ice will melt, water will become vapour and vapour will become water but the exact threshold cannot be predicted. All of the aforementioned changes are linked because they represent transitions of the system from one phase to another [19].
2.2 Phase transitions
In complex systems, phase transitions occur at thresholds or ‘tipping points’ that are characteristic of the system. The macroscopic phase transitions we witness are the result of small changes within the system. It is difficult to account for the macroscopic change in phase by observing the small changes witnessed at a microscopic level – but these abrupt transitions are due to the nonlinear relationships and interconnectedness between the different elements within the system [21].
Going back to the example of a phase transition of water turning to vapour, one can observe that at a certain range of temperatures, the water will heat up and then progress to an ordered simmering. As small and incremental amounts of heat continue to be added, there will come a point where the change in the movement of the water molecules is no longer ordered and it becomes chaotic as the simmering water transitions to a boil. This transition is continuous and it will only take a gradual increase in temperature to transition to a chaotic boil. The point at which this phase transition occurs is the threshold or ‘tipping point’ – a critical point at which “…the system is nearly unstable, with tiny disturbances possibly leading to global effects” – and demonstrates the emergent behaviour of complex systems [21].
Because of the nonlinear nature of complex systems, it is not possible to predict what the point of criticality will be and/or when a phase transition will occur. Furthermore, for complex systems that are self-organised, like organisations or our society more generally, the response of the system to external disturbances is even more difficult to predict because the response depends on the state of the entire system, which represents the history of inputs and responses to inputs within the system. When and how phase transitions occur and what the impact will be on the system as a whole as well as its individual elements represents a situation of fundamental uncertainty.
2.3 Fundamental uncertainty
In situations of fundamental uncertainty, like phase transitions, the outcomes that will result from a given set of inputs into a complex system are unpredictable and are too unique to allow for statistical analyses that can yield reliable probability estimates. Two important factors to account for in situations of fundamental uncertainty are that it is context-dependent and it is dynamic and not static. The context is important because though knowledge and methods to collect data on how different elements interact within a system at a microscopic level exist, this information does not yield insights to enable accurate predictions on outcomes within the system at a macroscopic level because of the dynamic and non-linear nature of the system. It is important to recognise this limitation to avoid classic problems of overfitting, where methods used to understand and manage risk are incorrectly used to address situations of fundamental uncertainty [22].
3. Fundamental uncertainty in the context of COVID-19 and its aftermath
3.1 Negative impacts of COVID-19’s aftermath
The COVID-19 pandemic will trigger phase transitions at multiple levels – individuals, communities, organisations, societies, states and globally. The negative impact of the pandemic will not, however, end with the acute effects we are currently witnessing. COVID-19’s aftermath will be equally as devastating and if we have learned from previous crises, it will take us many years to recover from it, particularly for the economic, education and health sectors.
The recessions triggered by the pandemic will have medium-long term impacts on the economy because of lower investment and fragmented global trade, which will dampen the global economic outlook resulting in a slower recovery for unemployment rates. This trend was also seen with the 2008 global financial crisis where unemployment rates took seven years to return to pre-2008 levels [1, 23]. It is important to note that the experiences of unemployment will be heterogeneously distributed with youth unemployment expected to be particularly high, a trend also seen with the 2008 global financial crisis [24]. Job losses and unemployment have long-lasting effects on the employment, earnings and income prospects of laid-off workers also leading to the ‘scarring effect’ for youth which leads to permanently lower earnings by ~1.2% per year for each additional month of unemployment [24, 25, 26].
For the education sector, simulations suggest that ~0.6 years of schooling will be lost globally due to school closures with the largest proportion occurring for children of lower socio-economic status [4]. This could have knock-on effects for these children with many at risk of never returning to school - studies suggest that ~24 million additional children and youth may drop out or not have access to school in 2021 [15, 16, 17, 18]. Effects on education of children and youth can extend beyond acute periods and produce negative impacts years later with models suggesting that students currently in school may lose $10 trillion in earnings over their work life if schools are closed for five months [4, 16, 17, 18].
Learning from previous crises, we know that the negative impacts on the economic and educational prospects of individuals will also have medium to long-term health consequences [2]. Unemployment and job insecurity are linked with several negative health outcomes including increases in all-cause mortality, death from cardiovascular disease and suicide and higher rates of mental distress, substance abuse, depression and anxiety [14, 24, 26, 27]. Nutritional deprivation of children and mothers can also negatively impact cognitive development of young children [4, 8].
Combined, these negative impacts on the economy, health and education of individuals and society will also increase inequalities and reduce social mobility. The largest welfare impacts will occur for the poorest households, which will lead to slower recoveries for them as well as unpredictable intergenerational effects - trends also seen with previous pandemics as well as the 2008 global financial crisis [1, 2, 3, 4, 26].
3.2 Fundamental uncertainty of the phase transitions triggered by COVID-19 and its aftermath
Given the wide-ranging impacts of the COVID-19 pandemic and its aftermath, it is not possible to predict exactly what will happen to individuals or systems. Acknowledging this fundamental uncertainty, it is also important to acknowledge another key characteristic of any complex system – namely that it will not be reversible to a pre-COVID-19 state. The reversibility of a complex system, particularly self-organised systems like the organisations and societies we create, is informed by the concept of hysteresis, which points to the importance of a particular phase on its history of inputs and responses to those inputs [28]. We can imagine our systems in a stable pre-COVID-19 state that is suddenly hit by COVID-19 which represents a shock to the system and drives it towards the system’s threshold and past its point of criticality to an unstable COVID-19 state. The unstable COVID-19 state will last for some time and as the acute effects of the COVID-19 pandemic subside, the system will stabilise and approach a stable post-COVID-19 stable state (Figure 1).
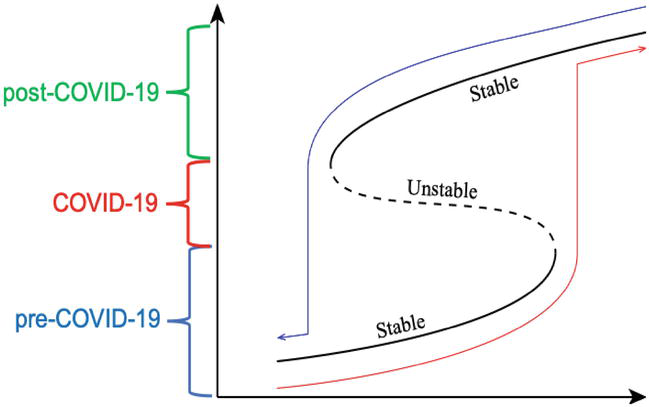
Figure 1.
Hysteresis-informed conceptualization of the COVID-19 pandemic and its aftermath. Hysteresis curve demonstrating how the transitioning stability from pre-post COVID-19 will lead to a new post COVID-19 stable state. The solid line in the curve indicates a stable state and the dashed line corresponds to an unstable state. (Figure 1 adapted, with permission, from reference [
Viewing our world through a complex systems-lens subject to hysteresis, it is important to note that a stable state only indicates that the system is not subject to unpredictable fluctuations experienced in response to systemic inputs that could lead to a phase transition – the stable state in this context does not indicate that the system is fair, equitable or equally beneficial for all elements of the system. Furthermore, once the system has reached the post-COVID-19 state, the irreversibility of our complex system will assert itself because we will not be able to go back to our pre-pandemic states – we will need to come to terms with a new ‘normal’.
4. Designing heuristics to cope with the fundamental uncertainty caused by COVID-19 and its aftermath
4.1 Heuristics in situations of fundamental uncertainty
When devising strategies to cope with the fundamental uncertainty thrust upon us by the COVID-19 pandemic, it is important to understand the distinction between situations of fundamental uncertainty and risk. In situations of risk, we have knowledge about how different variables interact and also have the ability to accurately and robustly measure, and often times predict, the impact of inputs into a system. In a situation of risk, more data will increase the ability to make predictions about outcomes. In a situation of fundamental uncertainty, however, more data can lead to the problem of overfitting. In these days of big data, there is a tendency to expect that more data will always be helpful and enable us to make better predictions. This holds true for situations of risk but not for situations of fundamental uncertainty where the outcomes of our actions are unpredictable and large amounts of data will only give one a false sense of security. This problem of overfitting was demonstrated recently at an international level with Google Flu trends [22, 30].
In situations of fundamental uncertainty, studies by Gigerenzer and other behavioural economists have shown that simple approaches known as heuristics can outperform complex algorithms based on big data models. Heuristics are strategies adapted to a decision-maker’s local context and can avoid overfitting, reduce resources required to make decisions while also supporting more accurate judgements by ignoring complexity, which can never be fully understood or controlled. Some examples of heuristics include the ‘1/N rule’ for investment where investors allocate resources equally to N alternatives to help to diversify portfolios and ‘satisficing’, where a decision maker explores alternatives and selects the first option that exceeds the decision-maker’s aspiration levels. In empirical studies, the ‘1/N rule’ has been shown to outperform optimal asset allocation portfolios and ‘satisficing’ has been shown to lead to better choices compared to chance [22].
4.2 Social determinants of health-informed heursitics in COVID-19’s aftermath
The COVID-19 pandemic and its aftermath represent nonlinear events that will drive phase transitions in fundamentally uncertain ways, and often times with negative outcomes. Despite the fundamental uncertainty decision-makers are facing, actions must be taken to try to reduce the negative impacts our citizens and societies face and, ideally, a more proactive approach should be taken to build a more sustainable, resilient, fair and equitable post-COVID 19 stable state. The ideal approach to cope with the changes we are seeing now and will see in the future is to design and implement appropriate heuristics but a key question that must be addressed is what these heuristics should focus on.
The heuristic we see being used across the world by many governments currently is to issue debt to support economies, healthcare systems and society more generally. While this has been the correct approach, it is important to recognise that the $24 trillion that has been introduced into our global systems is necessary but not sufficient to fully address the suffering our citizens will be facing now and in the future [1, 6, 7].
It is well established that 70–80% of health outcomes are due to social determinants of health, which include factors like access to housing, education, jobs, transportation, nutritious food, clean air, clean water, support services for substance misuse, support services to domestic abuse, etc. [31, 32, 33]. Heuristics designed to address social determinants of health at individual and societal levels will go a long way to improving resilience and supporting recovery and, ideally, preventing phase transitions to states of poor health whether that be at individual, organisational, societal, state or global levels. Actively promoting health, instead of just focusing on preventing disease, requires that we shift away from only focusing on the highest risk groups in our population to working to shift the entire risk profile to a lower risk status by addressing the factors that have the greatest impact on health – i.e. social determinants of health (Figure 2) [31, 32].
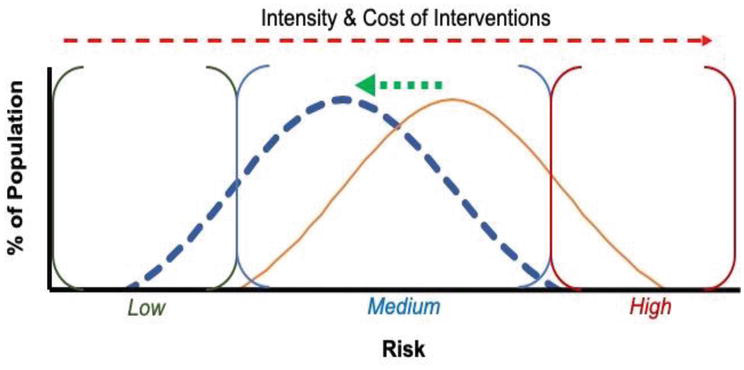
Figure 2.
Shifting risk profiles to promote health: Rose’s model of improving health by shifting risk profiles. The x-axis represents different risk subgroups going from low risk at the left to high risk at the right. To improve health, transitions (green arrow) must be made from the yellow bell-shaped curve to the blue dashed bell-shaped curve. Overlaid onto the different risk strata are the intensity and cost of intervention needed to prevent the strata from transitioning to states of ill health (red arrow above). (Figure 2 adapted, with permission, from reference [
In light of COVID-19’s negative impacts, it is even more imperative that we focus on social determinants which have such a large impact on health because it will not be possible to accurately predict the thresholds beyond which phase transitions into states of poor health will occur. Furthermore, once transitions have been made into higher risk groups and into states of poor health, the level of intervention needed to bring the systems back into a state of good health will be much higher and, in many cases, may be irreversible – i.e. for some individuals thrust into poverty, they will have difficulty escaping from poverty traps. Our best option is to promote resilience in the face of COVID-19 and doing so requires focusing on social determinants of health.
5. Promoting resilience in the face of COVID-19 and COVID-19’s aftermath
5.1 Resilience within complex systems
For complex systems, resilience entails progression to a new stable state and “…the resilience of a system is measured by the speed with which it returns to the stable fixed point” [21]. Resilience within complex systems is multidimensional and is supported by both internal and external factors. Focusing on health, external factors that can influence resilience rely heavily on social determinants, as described in Section 4. Internal factors for individuals and communities will also have an important role to play but they will often times be more subjective.
Every individual will have a different threshold at which they transition from states to health to lack of health or vice versa. Leveraging a contractualist perspective, individuals’ actions will be internally driven – information supporting their decisions can come from external sources, but an individual’s actions will be driven through internal processes of deliberation. These processes of deliberation see that an action:
The process of deliberation itself will be influenced by individual subjective motivational sets which are “dispositions of evaluation, patterns of emotional reaction, personal loyalties, and various projects, as they might be called, embodying commitments of the agent.” Subjective motivational sets can undergo various changes in response to an individual’s experiences, as well as external sources of information, and are important from a resilience perspective because they are the core driver for determining the approach an individual takes to bring themselves back to a stable state, notwithstanding the external influences that can support or constrain the individual’s progression to a stable state – in our case, to one of good physical and mental health [34].
To promote resilience, some broad approaches that can be taken are to [21]:
shift thresholds so that more inputs can be introduced into the system before a phase transition occurs;
to reduce extreme events that can introduce inputs that can drive phase transitions and/or
Create strategies that can adjust the pattern of input introduction into the system so that their potential destabilising impacts can be dissipated.
Approach 1 would be an ideal way of making our systems stronger and more resilient. At an individual level, they would require that we work to augment subjective motivational sets through education to drive individuals to engage more proactively in health-promoting activities. While very attractive, and ideal, it is difficult to create a standardised way to influence subjective motivational sets because they will be very heterogeneous within and across societies and across the individuals within a given society. This variability, in itself, introduces an important and unavoidable source of fundamental uncertainty.
Approach 2 would be great from a prevention perspective but, as COVID-19 has demonstrated, is out of our control in many cases. Approach 3 would rely on alternative mechanisms to dampen the potentially destabilising impacts of inputs into a system. For COVID-19, this would entail creating approaches to address the areas that will be impacted most and could increase the chances of individuals and societies transitioning to states of poor health. As discussed in Section 4, social determinants of health are an ideal starting point for building a set of interventions informed by Approach 3.
Given the fundamental uncertainty related to Approach 1 and the lack of control we have for Approach 2, this chapter will finish by providing a set of recommendations to promote resilience that focus on social determinants of health in a way that could help to dissipate the negative impact of the COVID-19 pandemic and its aftermath (Introduction and Section 3.1) and prevent transitions to poor states of health.
5.2 Social determinants of health-informed heuristics to promote resilience in response to COVID-19
COVID-19 has already had a substantial negative impact on individuals and societies, with some already transitioning to poor states of health. We know from previous crises that the trajectory of the future negative effects (Section 3.1) will affect the areas that can have the greatest impact on the short-, medium- and long-term health of individuals and populations. Three specific areas, which are captured within the broad domains of social determinants of health, are employment, education and health. To promote resilience in the face of COVID-19, addressing these areas will be an important mechanism to dissipate the impact of COVID-19 on our systems and subvert any potential phase transitions to states of poor health. We also know from previous crises that addressing these areas can dramatically affect recovery trajectories for dimensions of health as well as inequality [4, 26, 27].
5.2.1 Employment
For businesses, improving access to low-cost financial products can help them to survive and/or become more competitive, which could help to prevent unemployment at source, while also positioning them to create new jobs if they are able to become more competitive [4].
For struggling individuals and households, supporting them through augmented social welfare (e.g. furlough schemes) and benefits support schemes n(e.g. food vouchers for poor households) can help to keep them in a state of health for longer [1].
For those already unemployed, several approaches could be taken to prevent the negative long-term social and health-related effects of unemployment. Temporary income support in the form of unemployment insurance, redundancy payments and social assistance programmes can be provided to support displaced workers [4, 25, 27]. National job guarantee programmes with governments functioning as an ‘Employer of Last Resort’ through support of public works programmes such as green infrastructure (i.e. the ‘Green New Deal’) can create new jobs while also supporting and strengthening the wider economy [35]. Finally, active labour market programmes such as labour exchanges, education and training and support for subsidised employment programmes can help to support more people to get back into work [4, 25, 27].
5.2.2 Education
For interventions aimed at education, three focus areas can be to cope, manage continuity and then to more proactively work to improve and accelerate improvements to education systems to improve outcomes, address inequalities and reduce learning poverty [18].
Supporting education systems to cope and manage continuity in response to the COVID-19 pandemic is essential. In order to do so, school capacity should be strengthened to help schools reduce risks of disease transmission while also supporting mechanisms to ensure schools do not lose children, particularly vulnerable groups and students below learning proficiency standards, to drop-out. These approaches can include re-enrolment campaigns as well as cash transfer programmes [4, 18].
Some of the focus on changing education systems can also be directed to understanding approaches that can be taken to strengthen and accelerate improvements through investments to support teacher training, addressing any deficiencies in existing curricula and bolstering school infrastructure through technology-enhanced learning [18]. If designed and implemented well, these improvements can also include the introduction of methods to augment the subjective motivational sets of children and youth to help them choose health-promoting behaviours and make them more resilient (Approach 1, Section 5.1).
5.2.3 Physical and mental health
Programmes addressing core aspects of health will be essential. One of the most important will be to support food security through approaches like school meals and food subsidies to ensure we can avoid the short-, medium- and long-term negative consequences of malnutrition. In addition to this, where possible, using approaches like social prescribing to support individuals with conditions that can be brought into remission can help to promote health and also reduce demand on overstretched healthcare systems [36]. They also have the added benefit of supporting more health-promoting subjective motivational sets.
In addition to preventing transitions to ill health and supporting individuals to improve their health, healthcare systems will need to augment existing services with more staff and infrastructural support to provide care to those who are already ill and have not been able to access services and/or individuals who have acquired non-COVID-19 related illnesses during the lockdowns and have not been able to receive care. Given that we will also expect increased mental illness during and post-COVID-19, steps should be taken to prepare for this by raising awareness about mental health issues and also strengthening services such as hotlines and psychiatric services [3].
In the short term, identifying and supporting individuals at the highest levels of risk for falling ill can also be helpful in preventing acute and severe exacerbations of their existing conditions. This can be supported through social registries to ensure these individuals do not transition to states of severely poor health and to also track emerging risks within the population [4]. Caution must be taken with this approach, however, because it promotes an approach that addresses severe risk and preventing disease rather than actively promoting health (Figure 2).
6. Conclusion
The state of our post-COVID-19 future is uncertain and unpredictable. This can be very unsettling but, taken another way, it can also provide a sense of hope. Using the right approaches, we can use the opportunities given to us with the current drives to action to build a more sustainable, resilient, fair and equitable post-COVID-19 future. We will need to understand our constraints and be honest about where our ignorance lies so that we can take the most appropriate actions. A starting point for these actions should be to focus on social determinants of health because they have such a large impact on the health and wellbeing of individuals and societies more generally. As we progress to our post-COVID-19 state, some insights from Donella Meadows are helpful in keeping us humble, hopeful and focused as we look to continue to build our resilience:
References
- 1.
World Bank. The Global Economic Outlook During the COVID-19 Pandemic: A Changed World. See: https://www.worldbank.org/en/news/feature/2020/06/08/the-global-economic-outlook-during-the-covid-19-pandemic-a-changed-world (last checked 19 April 2021). - 2.
The Lancet Global Health Editors. Food insecurity will be the sting in the tail of COVID-19. The Lancet Global Health 2020; 8: E737. - 3.
Kawolh W and Nordt C. COVID-19, unemployment, and suicide. The Lancet Psychiatry 2020; 7: P389-P390. - 4.
World Bank Blogs. What COVID-19 can mean for long-term inequality in developing countries. See: https://blogs.worldbank.org/voices/what-covid-19-can-mean-long-term-inequality-developing-countries (last checked 19 April 2021). - 5.
The World Bank. Projected poverty impacts of COVID-19 (coronavirus). See: https://www.worldbank.org/en/topic/poverty/brief/projected-poverty-impacts-of-COVID-19 (last checked 19 April 2021). - 6.
Institute of International Finance. Global Debt Monitor. See: https://www.iif.com/Research/Capital-Flows-and-Debt/Global-Debt-Monitor (last checked 19 April 2021). - 7.
Reuters. COVID response drives $24 trillion surge in global debt: IIF. See: https://www.reuters.com/article/idUSKBN2AH285 (last checked 19 April 2021). - 8.
The World Bank. Food Security and COVID-19. See: https://www.worldbank.org/en/topic/agriculture/brief/food-security-and-covid-19 (last checked 19 April 2021). - 9.
Pan K-Y, Kok AAL, Eikelenboom M, Horsfall M, Jorg F, Luteijn RA, et al. The mental health impact of the COVID-19 pandemic on people with and without depressive, anxiety, or obsessive-compulsive disorders: a longitudinal study of three Dutch case-control cohorts. The Lancet Psychiatry 2020; 8: P121-P129. - 10.
Office for National Statistics. Coronavirus and depression in adults, Great Britain: June 2020. See: https://www.ons.gov.uk/peoplepopulationandcommunity/wellbeing/articles/coronavirusanddepressioninadultsgreatbritain/june2020 (last checked 19 April 2021). - 11.
Kim JU, Majid A, Judge R, Crook P, Nathwani R, Selvapatt N, et al. Effect of COVID-19 lockdown on alcohol consumption in patients with pre-existing alcohol use disorder. The Lancet Gastroenterology & Hepatology 2020; 5: P886-887. - 12.
Finlay I and Gilmore I. Covid-19 and alcohol—a dangerous cocktail. BMJ 2020; 369: m1987. - 13.
Sun Y, Li Y, Bao Y, Meng S, Sun Y, Schumann G, et al. Brief Report: Increased Addictive Internet and Substance Use Behavior During the COVID-19 Pandemic in China. Am J Addict 2020; 29: 268-270. - 14.
The World Bank. World Bank Education COVID-19 School Closures Map. See: https://www.worldbank.org/en/data/interactive/2020/03/24/world-bank-education-and-covid-19 (last checked 19 April 2021). - 15.
UNICEF. Education and COVID-19. See: https://data.unicef.org/topic/education/covid-19/ (last checked 19 April 2021). - 16.
The UN. Policy Brief: Educationduring COVID-19 and beyond. See: https://www.un.org/development/desa/dspd/wp-content/uploads/sites/22/2020/08/sg_policy_brief_covid-19_and_education_august_2020.pdf (last checked 19 April 2021). - 17.
UNESCO. Adverse consequences of school closures. See: https://en.unesco.org/covid19/educationresponse/consequences (last checked 19 April 2021). - 18.
World Bank Blogs. Learning losses due to COVID19 could add up to $10 trillion. See: https://blogs.worldbank.org/education/learning-losses-due-covid19-could-add-10-trillion (last checked 19 April 2021). - 19.
Meadows D. Thinking in Systems. Vermont, USA: Chelsea Green Publishing, 2008. - 20.
Marro J. Physics, Nature and Society: A Guide to Order and Complexity in our World. Switzerland: Springer, 2014. - 21.
Fieguth P. An Introduction to Complex Systems: Society, Ecology and Nonlinear Dynamics. Cham, Switzerland: Springer, 2017. - 22.
Mousavi S and Gigerenzer G. Risk, uncertainty, and heuristics. J Bus Res 2014; 67: 1671-1678. - 23.
Bank of England. How persistent will the impact of Covid-19 on unemployment be? See: https://www.bankofengland.co.uk/bank-overground/2020/how-persistent-will-the--impact-of-covid-19-on-unemployment-be (last checked 19 April 2021). - 24.
Grzegorczyk, M. and G. Wolff (2020) ‘The scarring effect of COVID-19: youth unemployment in Europe’, Bruegel Blog , 28 November - 25.
World Bank Group. Causes and Impacts of Job Displacements and Public Policy Responses. See: https://openknowledge.worldbank.org/bitstream/handle/10986/33720/Causes-and-Impacts-of-Job-Displacements-and-Public-Policy-Responses.pdf?sequence=1&isAllowed=y (last checked 19 April 2021). - 26.
Bambra C, Riordan R, Ford J and Matthew F. The COVID-19 pandemic and health inequalities. J Epidemiol Community Health 2020; 74: 964-968. - 27.
Hensher M. Covid-19, unemployment, and health: time for deeper solutions? BMJ 2020; 371: m3687. - 28.
Thom, René. Structural Stability and Morphogenesis: An Outline of a General Theory of Models. Reading, MA: Addison-Wesley, 1989. - 29.
Jani A and Kawazura Y. Policy responses to the nonlinear future of COVID-19’s aftermath. COVID: A complex systems approach [forthcoming 2021] - 30.
Lazer D, Kennedy R, King G and Vespignani A. The parable of Google Flu: Traps in big data analysis. Science 2014: 343: 1203-1205. - 31.
Rose G. Sick individuals and sick populations. Int J Epidemiol 1985; 14: 32-38. - 32.
Rose, G. A., Khaw, K.-T., & Marmot, M. G. (2008). Rose's strategy of preventive medicine: The complete original text. Oxford, UK: Oxford University Press. - 33.
WHO. Social Determinants of Health: the Solid Facts, 2nd edn. Geneva: WHO, 2003. - 34.
Scanlon TM. What we owe to each other. London: The Belknap Press; 1998. - 35.
Minsky HP. Ending Poverty: Jobs, not welfare. New York, NY: Levy Economics Institute, 2013. - 36.
Jani A, Gray M. Making social prescriptions mainstream. Journal of the Royal Society of Medicine 2019; 112: 459-461.