
Abstract
Under circumstances such as the COVID-19 pandemic, decompression is essential to slowly overcome the lockdown stressors as a transition period between lockdown and resuming work in a manner that is no longer going to be ‘business as usual’. Firstly, we examine what is decompression in the context of reducing overwhelming and unwanted pressure emanating from the pandemic. Secondly, we reiterate the objectives and goals of decompression. Thirdly, we list ways in which one can decompress as a suitable way of endowing us with better psychological and much needed emotional support in pandemic times. Finally, the chapter offers guidelines for future research as this aspect has not been researched much and opens up new avenues in the field of psychosocial research in civilian as well as military contexts which brings the need for psychological debriefing to the forefront. The results of psychological disaster research to foresee, reduce and soothe the psychological effects of mass disasters – in this case, the global COVID-19 pandemic, maybe reconstructive.
Keywords
- decompression
- post-traumatic growth
- pandemic
- reconstruction
- third-location decompression
1. Introduction
“Decompression fosters a means of progressively adjusting to a new normal, by allowing us to take a step back and reflect on the recent past before we leap ahead into unchartered waters of the future.” - Lt Col Dr Samir Rawat
Life is tough at Siachen glacier, in the Himalayas, India, the highest altitude battle zone in the world. A vast land spread over approximately 75 km, the glacier is deadly, because of sub-zero temperatures, frequent avalanches, high-altitude weather uncertainties, crevasses which go unnoticed, almost unimaginable and scary conditions for even soldiers to be. Soldiers deployed at the glacier typically spend three to four months in extreme conditions, highly vulnerable to fatal high altitude ailments like frost bites, chill blains and hypothermia. When soldiers return from active service in operational zones, they may find it difficult to immediately adapt to what seems to be a new reality now, they need some ‘time-off’ to adjust and acclimatize to out-of-operations conditions. Military psychologists [1], recommend a period of decompression- a release from compression, for soldiers returning from operational duties.
Given the adversity, the globe experienced in 2020, a global crisis of COVID-19 which ravaged the world order, destroyed poor and developed economies alike, exerted immense pressure on the mental health of people across the globe and pushed a whole civilization into nothing less than a warlike zone. The battle was with an unknown enemy- a virus that caught nations, societies and communities off-guard and thrust them into battle of survival. Traditional systems of social support, interpersonal relationships, easy access to resources became, which served as buffer to problems earlier, were challenged with most nations calling for lockdowns and social distancing as immediate strategies to curb the spread of the virus. This period has resulted in people losing control over their actions and emotions because of the suddenness and magnitude of change that the pandemic has brought in. Now, though the battle against the virus is far from over, we must move forward to normalcy, roll up our sleeves and put together strategies to bounce back- be adaptively resilient. Nearly a year long lockdown has exhausted our mental capacities, has been additionally difficult due to multiple roles that some of us are expected to take on, has changed how we approach life in general. For economies, global markets and multi-national organization, it has been a tough time and getting back to relative state of normalcy is a task that requires planning and organisation. Just as soldiers, when returning from the operational duties are allowed a period of decompression, a populace that has been wrecked by the pandemic be allowed a period of decompression.
2. Definitions
3. Decompression: an ally in reconstruction
In this article, we will introduce to the readers the concept of
A conceptual understanding of psychological decompression finds most mention in military literature; it refers to a process that allows soldiers returning from theatre of military operations and duties in war zones, to adapt to the home environment gradually, in a systematic manner with the aim to reduce the potential for maladaptive psychological well-being [2, 3]. Decompression is viewed as a period of transition between high-stress operational environment and home environment perceived to be relatively less stressful [3]. This organised period of transition is also known as third location decompression or TLD [4].
Psychological health issues experienced by soldiers returning from combat zone are well researched and documented. Highly volatile, ambiguous environments that theatre of operations are, exert mental pressure and stress on soldiers in spite of being trained in the use of arms and technological advances of militaries. Whether returning home victorious or mere deployment under volatile uncertain conditions or even peace-keeping operations, some amount of stress is innate and places them at higher risks for post-traumatic stress disorder, depression, alcohol or drugs abuse, and other co-morbidity conditions [5, 6, 7, 8, 9, 10]. Thus, with high vulnerability to post-traumatic stress disorders and related adjustment issues it seems reasonable that there is a period of relative adjustment to reduce the risks of full-scale disorders.
A period of psychological decompression with a focus on rest, cognitive and emotional reappraisal may a-part solution for soldiers after deployment along with psycho-educational interventions. In one of the studies [11], it was found that soldiers returning from war who got little time to decompress between off-operational duties and enrollment into inherently stressful academic environments, showed higher levels of academic stress than soldiers who got plenty or enough time to ‘get back to the center’. Shea [11] noted that soldiers who did not get time to adjust to roles like that of a parent, husband, kin in their families, if were put through additional pressures of academic stress, would experience stress the most and not perform as per expectations. In another study, [though not documented as an empirical study] of how decompression got charted into after-deployment or homecoming programs for militaries across the globe, is after the Falklands War in 1982, British military personnel reached back home by either of two ways—entirely by sea, meant an additional week to return home or they ferried their journey by sea and air. Press reports of the time suggested that the soldiers who travelled by sea route, and spent more time between the war and homecoming had better psychological health than those who made the trip in a shorter time [12].
3.1 Value of decompression
While engaging with the enemy on the ground, in the skies or even at sea are challenging environments, where military personnel go through immense psychological and mental changes, what could be as challenging, is to transition to environments that place different needs on their mental and psychological resources- like playing different roles, being available for their families, adjusting to non-combat environment. To successfully tread, they must bring about physical and psychological changes [13]. A line of thought also suggests that personnel returning from operational environments may in fact be happy about being home right after, however, at the cost of signs of mental health symptoms getting masked [14].
Though there is perhaps no absolute consensus on definitions of decompression and what comprises decompression programs, there is a general understanding that this period consists of rest, and restoration and should have psychologists or trained mental health professionals conduct psychological debriefing. There is a general belief that decompression should be closer or in close proximity to the unit or teams that were together in the operational tasks. We will discuss some of the aims of decompression in this section, namely, providing opportunity for emotional settling, a safe place to de-acclimatise, and an opportunity for structured debriefing to release tension.
Emotional decompression: combat or operational environments are marked by exposure to deprivation from resources, isolation and oftentimes, no communication with families for long spells, exposure to war atrocities that may result in acute or chronic psychosocial issues irrespective of the consequences of the operations [5, 15, 16]. The guilt of surviving when their colleagues suffered injuries or lay dead on the battlefield, anxiety about being away from the high-tension, sorrow could be some of the general emotional reactions. Some of these may go unnoticed or un-reported during or after deployment mainly because of the notions of military being a profession where emotions are not exhibited openly [17]. Similarly, emotions resulting from fear of being killed or due to degree of sustained injury [18] could also place individuals at higher risks of developing post-traumatic stress disorder or other adjustment issues [like substance abuse, depression, insomnia, cognitive overload, etc.]. Negative emotions are known to be detrimental to motivation, performance and sense of achievement not just in military but also in non-military environments [19, 20]. Thus, it becomes imperative that the negative emotions are acknowledged and strategies to manage these negative emotions such that these do not interfere with wellbeing, or spillover/displace to other areas of one’s functioning are made available. Third-location decompression is likely to provide with such much needed opportunities.
De-acclimatise: APA defines acclimatisation as adjustment or adaptation to new circumstances or environmental conditions, particularly the physiological changes that improve an individual’s ability to tolerate environmental alterations [21]. Extending on the element of adjustment or adaptation, we propose that decompression allows for de-acclimatization, which is to suggest that as the military or operational training trains the soldiers to be prepared for the volatility, vigilant, intense, sometimes dramatic nature of the battlefield; it is also, imperative that when the battle is over, soldiers unlearn some of the approaches to resilience and vigilance required during wartime and adapt to new realities and approaches for non-combat functioning.
Psychological debriefing: Research in the area of trauma and stress suggest that psychological debriefing has positive therapeutic effects for people with exposure to trauma and volatile conditions [22, 23, 24, 25]. Bartone and Adler [26] define debriefing [event-oriented after action debriefing] as a factual review of events, and reaction to events by the individual involved or the group/unit engaging in the events. In their classic research paper, they indicate the goals of debriefing to be—identification of lessons learned during operations which can direct actions in the future, resolve any misconceptions there could be, help soldiers paraphrase their battle experience positively, reduce sense of isolation and also make soldiers better aware of possible psychological symptoms resulting from stressful battle conditions.
Similar directions for the use or structure of debriefing are found in the work of Everly and Mitchell [2], who coined the term ‘critical incident stress debriefing’. According to CISD model [2], debriefing promotes emotional wellbeing by allowing opportunities for dialog to the soldier, where they can vent and work on their emotions, perceptions and appraisals of the critical events in the theatre of war. However, it is important to acknowledge that such expression of emotions can be overwhelming to soldiers, perhaps risking them to relive the events. Thus, the aim of psychological debriefing should be established and affirmed by psychologists and team leaders [or those who are close to the trauma context] before use to prevent this technique from being detrimental [27]. Post-mission debriefing sessions typically involve talking about critical or traumatic incidents during tour of duty [4]. While psychological debriefing may be seen as a viable technique for emergency responders, caregivers especially in the COVID times, the authors recommend the use of debriefing under strict vigilance and with caution, simply because pandemic has resulted in limited or depleted resources and the technique could in fact prove to be detrimental if missed shot. Debriefing could perhaps well be replaced with more effective techniques like cognitive therapy, mindfulness training [28, 29].
Fostering post-traumatic growth attitude: Decompression period can also be looked as a window of opportunity to foster growth-attitude among soldiers. Post-traumatic growth defined as positive and meaningful psychological change that an individual can experience after they have experienced a traumatic incident or event and are coping from it [30]. Though events like wars, or even calamities get associated with negative consequences, and changed worldviews, some may see these as opportunities to review their perceptions of world view before and after the events, restructure their thoughts and emotions and direct their action in order to grow, revitalize their self-concepts and relationships with others, from having experienced the events [31]. Thus, post-traumatic growth is essentially moving away from the baseline and toward growth in refurbishing the worldview, sense of control over what the future holds [31]. Research suggests that post-traumatic growth thoughts and attitudes are inversely related to post-traumatic stress symptoms [32, 33]. Decompression thus can be an important period when psychologists or professionals or team leaders can facilitate development of post-traumatic growth attitudes and cognitions. Post-traumatic growth perspective could prove useful in the post-COVID times with the virus having caused loss of enthusiasm and change in worldview with prolonged experiences of isolation, social distancing and uncertainty. For example, recent studies suggest emotional creativity, may result in post-traumatic growth attitude, thereby reduces the chances of full-blown post-traumatic stress disorder [34].
COVID-19 pandemic has brought about tectonic changes beyond the realm of imagination of most of societies, even for those who have experienced WW II, which so far was thought to be the most ravaging event of the century. Other epidemics [like SARS, plague, Ebola] and calamities have not had the magnitude of impact and consequences that COVID-19 has caused. Thus, it becomes essential that the available knowledge of the past from crisis management experiences be remodeled, reinvented and re-adapted to suit what may fit the bill for reconstruction post-COVID crisis.
3.2 Psychological consequences of covid-19 pandemic
Why a discussion on decompression becomes important lies in the spectrum of psychological, social and interpersonal impact COVID-19 virus has brought about. COVID-19 presents before us the most-multifaceted crisis the human race has seen, a battle where the enemy is unknown and unseen. No amount of intelligence and force mobilization can fully avert the mayhem that the virus resulted in. With some common knowledge or best described as available knowledge of how spread of the virus can be curtailed, governments across the world imposed lockdown of economies, restrictions on movement, curb of social and interpersonal interactions and what seemed to be business as usual was no longer the same. Medically, the rapid infection and contagion resulted in strained medical systems. Economically, it meant businesses were thrown into fiscal deficits and societies were propelled into threats of destabilisation and loss of normalcy. Beyond the socio-economic disaster that the pandemic has been, psychological impact has been beyond comprehension and indisputable [35, 36]. Research suggests that fear of the pandemic and its uncertain nature could be a precursor to stress disorders, anxiety and other related problems, depression and even substance abuse [37]. With businesses being affected, it has resulted in people losing their source of livelihood and thereby adds to the stress of managing families. These could have potentially triggered related problems of substance abuse and panic disorders [38]. For emergency responders, this has been a period of turmoil, both professionally and personally. Long working hours, limited resources, worries about those affected, fear of being infected, inadequate access to basic resources, not being allowed to meet own families, being continuously in the line of action, suddenly being forced into harm’s way has all resulted in psychological distress [39].
A general environment of despair and loss of hope has resulted from the experience of loss of loved ones or witnessing death in close proximity or sense of being lost. Being home bound or quarantined has resulted in sense of loneliness and isolation and curtailed scope of human-to-human interaction or social support. Measures put in place as first reaction to curb spread of virus like lockdown and social distancing are likely to result in far-reaching psychological problems which may keep brewing on the inside and erode the very fabric of human civilisation more than the damage caused by the virus itself. Thus, it has been nothing short of a psychological warfare.
Yet, in all this, it is important to acknowledge that survival instinct is innate in the human race and while the pandemic might have bogged down the spirit, the ability to bounce back higher and with far greater strength also are innate. Further to the discussion on post-traumatic growth, the application of the same may be exemplified in times to come. New learning gathered from the pandemic can be put to use to develop habits and systems which are resilient as well wean off behaviors (like addictions, behaviors detrimental to general hygiene, burnout at work, pollution, etc.) which are detrimental in survival of the species.
4. 9-R model of decompression for war-at-hand
Most of decompression programs, as they exist in military organisations, agree on some of the core fundamentals like—belief that soldiers need some time-off after high-tension deployment, having collective decompression opportunities for those who experience challenging operations, providing for individual and group unwinding–rewinding sessions and focus of relaxation and rest. The aim of decompression programs is to restore and regain resilience in soldiers, authors of this article seek to provide and facilitate movement of societies, communities and organisations toward post-pandemic resilience and remodeling of mental capacities. The authors of this article, from their own experience of serving in the high-emotions theatre of war, volatile and uncertain battle grounds, as well as detailed research and empirical data (both internet data and personal communication) propose a nine-component model or 9-R model of decompression, see Figure 1. Authors also state firmly that an individual’s willingness and urge to change the status quo, resources available, learn new coping and adapt with resilience lie at the centre or core of any effective program.
Rest: Rest which can be understood as ceasing of any movement or activities in order to recover strength, especially after stressful event. Rest is a vital for better mental and physical health and people recovering from strains and illnesses are advised to observe period of rest to reinstate health and wellbeing [40, 41, 42]. Human downtime, is important not just for survival, but also for creativity and innovation. A period of rest could help individuals to break the chain of negative thoughts and habits they may have developed during the pandemic and develop new ways to move into new reality with a sense of growth and resilience [43].
Relaxation: relaxation defined as an emotional state of low tension, marked by absence of arousal [resulting from anger, fear, anxiety] is much researched and approved technique in stress management [44, 45]. Relaxation if practised consciously or mindfully is likely to result in reduction of physical and psychological stress. Empirical data suggest that relaxation- physical and mindful mental relaxation results in lowered anxiety levels during pandemic [36]. Relaxation can have benefits like normalizing heart rate, better sleep, lower fatigue, reduce muscle tension, most of which could be the result of heightened levels of anxiety for soldiers after deployment in warzone or COVID warriors with changes in their life circumstances.
Recognize achievement: Recognize one’s own and other’s achievement: In times like the pandemic or even battles, sense of self-worth and self-concepts may go through a sort of shift because the outcomes, personal loss, depletion of resources, and isolation. Dolan and Sanchez [46] suggest that in such times, being overly critical of oneself or others may be detrimental. A soldier who may have lost some of his fellow colleagues in the battle could already be struggling with guilt of survival or loss of a dear family member, may result in self-doubt of the caregiver. In such times, appreciation of their effort, could help in reinstating their belief in self-worth.
Reduce stigma: Stigma as defined by Goffman [47] is an attribute, of discrediting, reducing a person from a whole and usual person to a tainted, discounted one. By and large, intense situations like fighting a war or being involved in high-tension situations may be associated with a sense of bravado, valour and grit, there are certain inherent expectations especially and traditionally of how soldiers need to be—not come across as ones exhibiting emotions, being a team player. While most of these expectations may be occupational requirement, any deviation in following the same may have stigma attached to it. Decompression should be viewed as a period when such soldiers are provided with assistance to overcome fear of being stereotyped and steer clear any such detrimental thoughts they may have. In 2020, when most of the nations experienced the wrath of the virus, emergency first responders like medical professionals, doctors, police, pharmacos were the first to respond, which also placed them at a higher risk of infection and the risk of infection may get associated with stigma [48]. For instance, since the epicenter of the virus was located in one of the Asian countries, there were cases of discrimination being reported against foreigners of Asian origin [49, 50]. The debilitating effects of stigma place patient or affected groups of people at risk of being discriminated and isolated and thus lead to more psychological concerns. Now that societies take time to reflect before plunging into the future, measures should be taken to reduce the stigma and make available psychological assistance for people who could be at higher risks or being discriminated.
Regulated response: the pandemic has posed unique and unexpected challenges and health risks that place additional pressure on our coping resources. Collective restraint and control will enable our ability to curb the spread of the infection. The self-regulatory approach includes cognitive and emotional skills that allow us to intentionally control thoughts, emotions, and behavior [51]. A soldier’s ability to regulate during operations and even peace-keeping operations [which partly comes from military training], is critical to in sustaining military prudence and conforming to military norms and standards [52]. Decompression could be viewed as a period to strengthen self-regulatory habits such that soldiers restrain or control any spillover of negativity or other emotions like performance anxiety, extreme caution from highly charged combat environments into relatively docile family, interpersonal and social environments. Just like how soldiers are expected to observe restraint in their reactions, emotions, the pandemic has placed a demand on the civilian societies to control and manage their actions- like restrained movement, measures of hygiene, controlling substance abuse, etc. When working professionals return to workplace, it could be required of them to continue to observe limited interactions with their colleagues and also follow protocols such that they do not place themselves or others in the harm’s way.
Reflection: self-reflection is defined as an ability to willingly learn more about one’s fundamental purpose and to willingly exercise introspection [53]. As the world witnesses, almost a full range of change for example reorganization of lifestyle during and after the pandemic an ability to reflect on one’s thoughts, feelings and actions would be imperative [54]. During the decompression phase, reflection can help, steer clarity about the perceptions of the situation and how one approaches the change process. Reflection could be effective especially after a critical incident when certain milestones have been achieved or when one is trying to make sense of available information. A simple reflection of which habits [like social distancing, no smoking] helped in minimizing the effects of the virus or for soldiers reflecting on how training worked effectively during operations could go a long way in directing actions and thoughts for the future.
Reintegrate: any crisis brings with it some degree of loss of equilibrium. Golan [55] refers to a crisis as a sequence of events leading the movement from lack of equilibrium or disequilibrium to the state of equilibrium. Right after a war is fought or in this case a psychological war which is far from over, the definition of reality which existed has been challenged. Thus, as we take some time out, it is important that we re-assess the meaning and purpose of new reality and how best we respond to the changes that are resulting from a fairly long period of disruption. Reintegration would likely require making conscious changes in self and environment, organizations and communities. For example, organizations are putting together robust rehabilitation plans for employees coming back to work, religious communities which provided assistance to their members through meetings and congregations are moving to online modes of communication, etc.
Reboot: Albert Einstein exclaimed that in the midst of every crisis lies great opportunity. This crisis though has been an unsolicited one, has brought to the fore that issues like climate change, global healthcare systems, medical and scientific advances, need to dealt with foremost priority and shared responsibility among nations and global institutions which were caught off guard. Just as when soldiers return from theatre of war, can use their experience—how they survive with limited resources, how they follow a disciplined life, being vigilant; these life skills could be most beneficial to the non-military world which is dealing with the crisis. The pandemic with its mulling consequences of loss, grief and negative emotions has changed behaviours and thoughts which could be detrimental, for example, loss of a family member could make an individual overly cautious or being isolated could result in an individual showing asocial traits and other altered behaviors. These consequences may go unnoticed, however, could covertly damage the fabric of human interactions. It is a right time to slam hard on the reset/reboot button and aim at building conducive transition models holistically.
Reconstruction: Reconstruction in Myer and Zunin’s ‘Phase of Disaster’ theory [56] marks the stage of new beginning. This phase according to the theory is marked by individual and community effort to rebuild their lives while continuing to grieve the losses. Reconstruction particularly is the phase of recovery or conscious effort to move toward state of recovery. Most of the nations have now begun their journey of recovery, a pandemic-like crisis, which requires collective force mobilization efforts on the part of developed nations- in form of providing the necessary resources and developing nations and poorer economies to use this time to build stronger and sustainable systems for better future.
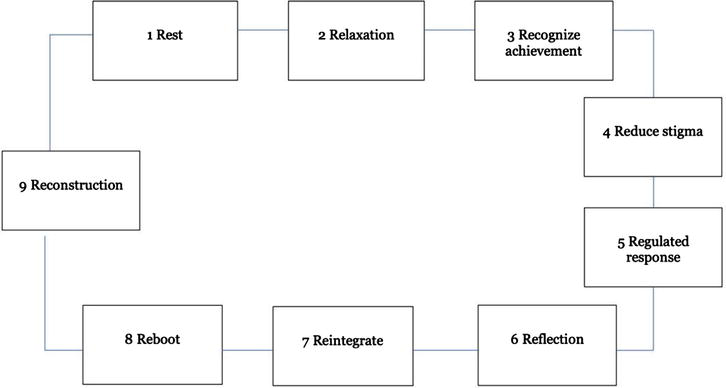
Figure 1.
9-R model of decompression.
The authors hope and assert that the model will prove a new direction in our endeavour to move toward re-integration and reconstruction of what lay in front of us as a new reality now that it becomes evident that moving to relative normalcy as a necessity for sustenance of the civilization. The 9-R decompression model aims to be a start point for future research and development into strengthening our understanding of how to manage the effects of combat and war fatigue. The period of decompression may vary from person to person and like in counselling, eclectic or customized approach may be an apt pick to deal with individual’s socio-economic and psychological build.
5. Conclusion
In conclusion, the authors of the article promote the benefits of having a period of transition, between the social isolation that people around the globe have been forced to and going back to work or new reality. However, as psychologists and responsible leaders, it is also important to create awareness of the nature and the process of decompression, for it to be effective. Some research results suggest that if this transition is considered prolonged, this could have a negative impact on health and well-being of the individuals [57], thus caution and communication should be prioritized for decompression to be effective.
Decompression seems to be a viable solution given the necessity to tread being well and with relatively less damage to the foundation of the societies, organizations and communities. Thus, decompression programs need to be tailored to suit the requirements and could be coupled with other effective techniques and approaches—like post deployment longitudinal screening [58, 59], trauma-focused cognitive therapy [60] which have proven as if not more effective in managing psychological and physical wellbeing in the aftermath of a crisis.
Finally, the authors also acknowledge that thriving through calamities and disasters perhaps is partly innate. As a civilization, even when we face catastrophe like COVID-19 of sorts we are engineered in a way to sustain and thrive and some of us are likely to show exceptional courage and grit to turn a tragedy into testimony of progress and success and show the lead to way into a new future.
References
- 1.
Piotrowski A, Boe O, Rawat S, Bergh J. Significant value of decompression on lifting of lockdown during pandemic—Follow 9 R’s. In: Military Psychology Response to Post-Pandemic Reconstruction. Jaipur, India: Rawat Publications; 2020. pp. 498-516 - 2.
Everly GS, Mitchell JT. A primer on critical incident stress management (CISM). The International Critical Incident Stress Foundation; 2003 - 3.
Hacker Hughes JGH, Earnshaw NM, Greenberg N, Eldridge R, Fear NT, French C, et al. The use of psychological decompression in military operational environments. Military Medicine. 2008; 173 (6):534-538 - 4.
De Soir E. Psychological adjustment after military operations: The utility of postdeployment decompression for supporting health readjustment. In: Bowles SV, Bartone PT, editors. Handbook of Military Psychology: Clinical and Organizational Practice. Cham: Springer International Publishing; 2017. pp. 89-103. DOI: 10.1007/978-3-319-66192-6_7 - 5.
Fear NT, Jones M, Murphy D, Hull L, Iversen AC, Coker B, et al. What are the consequences of deployment to Iraq and Afghanistan on the mental health of the UK armed forces? A cohort study. Lancet. 2010; 375 (9728):1783-1797 - 6.
Dedert EA, Green KT, Calhoun PS, Yoash-Gantz R, Taber KH, Mumford MM, et al. Association of trauma exposure with psychiatric morbidity in military veterans who have served since September 11, 2001. Journal of Psychiatric Research. 2009; 43 (9):830-836 - 7.
Adamson DM, Burnam MA, Burns RM, Caldarone LB, Cox RA, D’Amico EJ, et al. Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist recovery. RAND Corporation. 2008. Available from: https://www.rand.org/pubs/monographs/MG720.html - 8.
Grieger TA, Cozza SJ, Ursano RJ, Hoge C, Martinez PE, Engel CC, et al. Posttraumatic stress disorder and depression in battle-injured soldiers. The American Journal of Psychiatry. 2006; 163 (10):1777-1783 quiz 1860 - 9.
Stimpson NJ, Thomas HV, Weightman AL, Dunstan F, Lewis G. Psychiatric disorder in veterans of the Persian Gulf War of 1991. Systematic review. The British Journal of Psychiatry. 2003; 182 :391-403 - 10.
Kelsall H, Sim M, Forbes A, Glass D, McKenzie D, Ikin J, et al. Symptoms and medical conditions in Australian veterans of the 1991 Gulf War: Relation to immunisations and other Gulf War exposures. Occupational and Environmental Medicine. 2004; 61 (12):1006-1013 - 11.
Shea KP. The effects of combat related stress on learning in an academic environment. 2010. Available from: https://krex.k-state.edu/dspace/handle/2097/6683 - 12.
Schell TL, Farris C, Miles JNV, Sloan J, Scharf DM. The Air Force Deployment Transition Center: Assessment of Program Structure, Process, and Outcomes. Rand Health Q. 2017; 7 (1):7 - 13.
Zamorski M, Britt TW. The psychology of transition: Adapting to home after deployment. In: Adler AB, editor. Deployment Psychology: Evidence-Based Strategies to Promote Mental Health in the Military. Washington, DC, USA: American Psychological Association; 2011. pp. 153-174 - 14.
Bliese PD, Wright KM, Adler AB, Thomas JL, Hoge CW. Timing of postcombat mental health assessments. Psychological Services. 2007; 4 (3):141-148 - 15.
Allison-Aipa TS, Ritter C, Sikes P, Ball S. The impact of deployment on the psychological health status, level of alcohol consumption, and use of psychological health resources of postdeployed U.S. Army Reserve soldiers. Military Medicine. 2010; 175 (9):630-637 - 16.
Vasterling JJ, Proctor SP, Friedman MJ, Hoge CW, Heeren T, King LA, et al. PTSD symptom increases in Iraq-deployed soldiers: Comparison with nondeployed soldiers and associations with baseline symptoms, deployment experiences, and postdeployment stress. Journal of Traumatic Stress. 2010; 23 (1):41-51 - 17.
Hoge CW, Castro CA, Messer SC, McGurk D, Cotting DI, Koffman RL. Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. The New England Journal of Medicine. 2004; 351 (1):13-22 - 18.
Hoge CW, Terhakopian A, Castro CA, Messer SC, Engel CC. Association of posttraumatic stress disorder with somatic symptoms, health care visits, and absenteeism among Iraq war veterans. The American Journal of Psychiatry. 2007; 164 (1):150-153 - 19.
Pekrun R, Goetz T, Daniels LM, Stupnisky RH, Perry RP. Boredom in achievement settings: Exploring control–value antecedents and performance outcomes of a neglected emotion. Journal of Educational Psychology. 2010; 102 (3):531-549 - 20.
Zeidner M. Anxiety in education. In: International Handbook of Emotions in Education (Educational Psychology Handbook Series). New York, NY, USA: Routledge/Taylor & Francis Group; 2014. pp. 265-288 - 21.
American Psychological Association. Acclimatization—APA Dictionary of Psychology [Internet]. 2020. Available from: https://dictionary.apa.org/acclimatization - 22.
Auxéméry Y. Treatment of post-traumatic psychiatric disorders: A continuum of immediate, post-immediate and follow-up care mediated by specific psychotherapeutic principles. Clinical experience in French-speaking countries. Encephale. 2018; 44 (5):403-408 - 23.
Campfield KM, Hills AM. Effect of timing of critical incident stress debriefing (CISD) on posttraumatic symptoms. Journal of Traumatic Stress. 2001; 14 (2):327-340 - 24.
Dolan N, Tedeschi C. A qualitative study of psychological outcomes in avalanche first responders. High Altitude Medicine & Biology. 2018; 19 (4):344-355 - 25.
Smith MH, Brady PJ. Changing the face of Abu Ghraib through mental health intervention: U.S. Army Mental Health Team conducts debriefing with military policemen and Iraqi detainees. Military Medicine. 2006; 171 (12):1163-1166 - 26.
Bartone PT, Adler AB. Event-Oriented Debriefing Following Military Operations: What Every Leader Should Know. Europe: US Army Medical Research Unit; 1995 Report No.: WRAIR/TR-95-0017 - 27.
van Emmerik AAP, Kamphuis JH, Hulsbosch AM, Emmelkamp PMG. Single session debriefing after psychological trauma: A meta-analysis. Lancet. 2002; 360 (9335):766-771 - 28.
van der Riet P, Levett-Jones T, Aquino-Russell C. The effectiveness of mindfulness meditation for nurses and nursing students: An integrated literature review. Nurse Education Today. 2018; 65 :201-211 - 29.
Ghawadra SF, Abdullah KL, Choo WY, Phang CK. Mindfulness-based stress reduction for psychological distress among nurses: A systematic review. Journal of Clinical Nursing. 2019; 28 (21-22):3747-3748 - 30.
Zoellner T, Maercker A. Posttraumatic growth in clinical psychology—A critical review and introduction of a two component model. Clinical Psychology Review. 2006; 26 (5):626-653 - 31.
Tedeschi RG, Calhoun LG. Target article: “Posttraumatic growth: Conceptual foundations and empirical evidence”. Psychological Inquiry. 2004; 15 (1):1-18 - 32.
Dunigan JT, Carr BI, Steel JL. Posttraumatic growth, immunity and survival in patients with hepatoma. Digestive Diseases and Sciences. 2007; 52 (9):2452-2459 - 33.
Iversen AC, van Staden L, Hughes JH, Greenberg N, Hotopf M, Rona RJ, et al. The stigma of mental health problems and other barriers to care in the UK Armed Forces. BMC Health Services Research. 2011; 10 (11):31 - 34.
Zhai H-K, Li Q , Hu Y-X, Cui Y-X, Wei X-W, Zhou X. Emotional creativity improves posttraumatic growth and mental health during the COVID-19 pandemic. Frontiers in Psychology. 2021; 3 (12):600798 - 35.
Fagiolini A, Cuomo A, Frank E. COVID-19 diary from a psychiatry department in Italy. The Journal of Clinical Psychiatry. 2020; 81 (3):20com13357 - 36.
Ozamiz-Etxebarria N, Idoiaga Mondragon N, Dosil Santamaría M, Picaza GM. Psychological symptoms during the two stages of lockdown in response to the COVID-19 outbreak: An investigation in a sample of citizens in Northern Spain. Frontiers in Psychology. 2020; 18 (11):1491 - 37.
Shigemura J, Ursano RJ, Morganstein JC, Kurosawa M, Benedek DM. Public responses to the novel 2019 coronavirus (2019-nCoV) in Japan: Mental health consequences and target populations. Psychiatry and Clinical Neurosciences. 2020; 74 (4):281-282 - 38.
Qiu J, Shen B, Zhao M, Wang Z, Xie B, Xu Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatr. 2020; 33 (2):e100213 - 39.
World Health Organization. Mental health and psychosocial considerations during the COVID-19 outbreak [Internet]. Report No.: WHO/2019-nCoV/MentalHealth/2020.1. World Health Organization; 2020. Available from: https://apps.who.int/iris/handle/10665/331490 - 40.
Svenson BE. Identification and elucidation of fields of research within health and social training courses of medium length. Interdiciplinaria. 1990; 9 :41-53 - 41.
Asp M. Rest. Global Qualitative Nursing Research. 2015; 2 :2333393615583663 - 42.
Han B-C, Wallin O. Trötthetssamhället. Stockholm: Ersatz; 2016 - 43.
Chawla N, MacGowan RL, Gabriel AS, Podsakoff NP. Unplugging or staying connected? Examining the nature, antecedents, and consequences of profiles of daily recovery experiences. Journal of Applied Psychology. 2020; 105 (1):19-39 - 44.
Corliss J. Six relaxation techniques to reduce stress. Harvard Health. 2016. Available from: https://www.health.harvard.edu/mind-and-mood/six-relaxation-techniques-to-reduce-stress - 45.
Yanilov E, Boe O. Krav Maga: Combat Mindset & Fighting Stress: How to Perform under Alarming and Stressful Conditions. London: Meyer & Meyer Sports Ltd; 2020 - 46.
Dolan SL, Sanchez SG. Covid-19, stress, self-esteem, values, and psychological well-being: How to assess risks of becoming depressed, anxious, or suicidal? The European Business Review. 2020. Available from: https://www.europeanbusinessreview.com/covid-19-stress-self-esteem-values-and-psychological-well-being-how-to-assess-risks-of-becoming-depressed-anxious-or-suicidal/ - 47.
Goffman E. Stigma: Notes on the Management of Spoiled Identity. Reissue ed. New York: Touchstone; 1986 168 p. - 48.
Abdelhafiz AS, Mohammed Z, Ibrahim ME, Ziady HH, Alorabi M, Ayyad M, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). Journal of Community Health. 2020; 21 :1-10 - 49.
Coste V. Coronavirus: France faces “epidemic” of anti-Asian racism [Internet]. Euronews. 2020. Available from: https://www.euronews.com/2020/02/03/coronavirus-france-faces-epidemic-of-anti-asian-racism - 50.
Haynes S. As coronavirus spreads, so does xenophobia and anti-Asian racism [Internet]. Time. 2020. Available from: https://time.com/5797836/coronavirus-racism-stereotypes-attacks/ - 51.
Boud D, Keogh R, Walker D. Promoting Reflection in Learning A Model. Reflection Turning Reflection into Learning. London: Routledge; 1985 References - Scientific Research Publishing [Internet]. Available from: https://www.scirp.org/%28S%28czeh2tfqyw2orz553k1w0r45%29%29/reference/referencespapers.aspx?referenceid=1434298 - 52.
Carver CS. Self-awareness. In: Handbook of Self and Identity. New York, NY, USA: The Guilford Press; 2003. pp. 179-196 - 53.
Blair C, Raver CC. Individual development and evolution: Experiential canalization of self-regulation. Developmental Psychology. 2012; 48 (3):647-657 - 54.
Rawat S. COVID-19: Showing resilience through self-regulation [Internet]. https://www.outlookindia.com/ . 2020. Available from:https://www.outlookindia.com/newsscroll/covid19-showing-resilience-through-selfregulation/1785928 - 55.
Golan N. Treatment in Crisis Situations (Treatment Approaches in the Human Services). Bradford, UK: Stephen White Books; 1978. Available from: https://www.abebooks.co.uk/9780029120606/Treatment-Crisis-Situations-Approaches-Human-0029120608/plp - 56.
Myers D, Zunin L. Phases of disaster. In: Training Manual for Mental Health and Human Service Workers in Major Disasters. Washington, DC: DHHS Publication, Department of Health and Human Services; 2000 - 57.
Buckman JEJ, Sundin J, Greene T, Fear NT, Dandeker C, Greenberg N, et al. The impact of deployment length on the health and well-being of military personnel: A systematic review of the literature. Occupational and Environmental Medicine. 2011; 68 (1):69-76 - 58.
Dunt D. Review of Mental Health Care in the Australian Defence Force and Transition Through Discharge. Department of Veterans’ Affairs; 2019. Available from: https://www.dva.gov.au/documents-and-publications/review-mental-health-care-australian-defence-force-and-transition - 59.
Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA. 2006; 295 (9):1023-1032 - 60.
Bisson JI. Post-traumatic stress disorder. BMJ. 2007; 334 (7597):789-793