
Abstract
This manuscript aims to discuss the experiences and expectations regarding the cultural competence of Brazilian CSD students and the challenges brought by the COVID-19 pandemic. Cultural awareness has been one of the competencies focused on by CSD programs in Brazil. However, travel and face-to-face contact with persons from different cultures and environments is just one of the possible ways of experiencing cultural awareness. The interruption of these opportunities due to the COVID-19 pandemic did not reduce the interest in learning and improving cultural abilities. It is possible to think about alternatives for embedding discussions and experiences regarding cultural sensitivity in students’ routine studies and practice.
Keywords
- COVID-19 PANDEMIC
- cultural competence
- communication sciences and disorders
- Brazil
1. Introduction
This chapter aims to bring information and consideration regarding cultural competence as part of the education of the professionals that work with Communication Sciences and Disorders in Brazil. The first important information is that this professional is called Phonoaudiologist and has habilitation both in Speech and Language and in Audiology.
Phonoaudiologist is the professional with higher education that works in the area of Communication Sciences and Disorders. In all Latin America the areas of Audiology (assessment and rehabilitation of hearing and hearing disorders) and Speech-Language Therapy (assessment and intervention with communication, voice and swallowing disorders) are the professional field of Phonoaudiology.
Another major aspect that must be brought to attention is the complexity of the country. The authors will present some information about Brazil as a country and the current issues that are most relevant to the discussion of how cultural competence is considered in the education of Phonoaudiologists and the impact of COVID-19 in this regard.
It is easy to understand that the overview about Brazil will be superficial and incomplete, as would happen with any other attempt to synthesize important aspects such as the history, geography, and economy of a country in just a few paragraphs.
2. Brazil: some information about the country
What is nowadays the country of Brazil was a Portuguese colony from the sixteenth century until the nineteenth century. The formation of its people and society was the result of the genocide of the original population, the enslavement, and forced immigration through the kidnapping of African individuals aiming to boost the colony’s economic workforce based on the extractivist agriculture [1]. During the three centuries of slavery, almost 4 million persons were forcibly brought from Africa to Brazil [2]. These groups, added by the European colonizers, brought different cultural elements that are now an intrinsic part of Brazilian culture in areas such as food, religion, music, and language [3].
When slavery came to an end there was no official segregation, but structural racism still can be observed. It is clear in the small numbers of African descendants in universities, or higher positions in the workforce or political posts—when the topic is black women, the lack of possibilities is even bigger. Albeit several debates have been dedicated to the racial question in Brazil, including the famous idea of a racial democracy [4], this is still a sensitive issue generating social gaps in different and complex levels of the Brazilian society in major cities as well as in small and distant towns.
Structural racism is defined as a social, economic and politic system where institutional and public policies reinforce and maintain the segregation and inequities of social groups based on ethnicity, race or “color.”
The “whitening” process that the Brazilian population went through during the nineteenth and twentieth centuries, with the arrival of different groups of immigrants, mainly from Europe, the Middle East, and Japan, was a National State Policy and helped in the deepening of racial and social inequalities. Its reflexes are seen until the present day. Figure 1 shows the origins of the 4.3 million immigrants that arrived in Brazil during the nineteenth century.
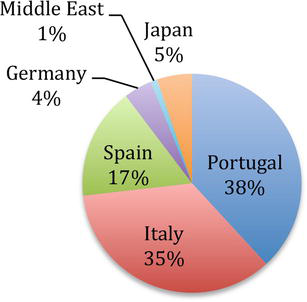
Figure 1.
Imigrants during the nineteenth century.
Brazil is the 5th largest country in the world and there are also enormous geographic contrasts. The largest cities are located in the southeast, a very industrialized region that concentrates almost 55% of the country’s entire gross product and 42% of the population. For example, São Paulo is the largest city, with over 12.3 million inhabitants; Rio de Janeiro has a demographic density of over 5.6 thousand inhabitants per square kilometer. The north and central regions are the most rural and preserved areas, despite the recent reduction of environmental preservation policies. In the Amazon region, the state of Roraima has the lowest demographic density in the country, with 2.33 inhabitants per square kilometer.
Immigration and migration processes are also different in different regions and at various moments, with different cultural impacts. During the last decade, the number of immigrants arriving in Brazil has increased from 17,188 in 2010 to 117,037 in 2020 [2]. Figure 2 shows the origins of the largest groups of immigrants to Brazil in the last decade.
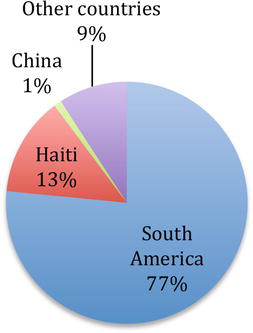
Figure 2.
Immigrants in the last decade.
Their distribution in the different regions of the country is shown in Figure 3.
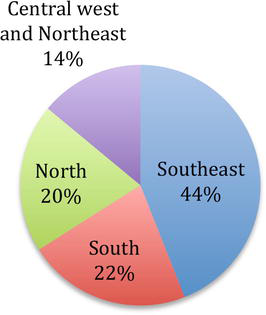
Figure 3.
Distribution in the different regions.
Brazil has many and large cultural, social, environmental, economic, and educational differences. Portuguese is the official language, spoken by the whole population (over 213 million), but there are large differences associated with specific regions of the country, traditions, age groups, and other aspects.
The original populations are still another aspect of Brazilian diversity. Of the almost 1 million persons of indigenous origin, 60% live in protected areas designated by the federal government. The North region has the largest indigenous population and there are 305 different ethnic groups that speak 274 different languages [5].
It becomes clear that cultural differences are, historically, a relevant part of Brazilian society. Therefore, all the major universities have “Culture and Extension” offices that encourage and support initiatives directed toward the integration between the universities and the specific society where they are located. This way, different actions are carried out in different universities aiming to better reach the different groups. This includes the programs in the areas of communication sciences and disorders.
Culture and Extension offices in the universities usually have a mission statement of bringing together the university and the environment and community where it is located. The activities are usually as diverse as developing educational experiences to children of different groups to expand sports technology, or from providing health assistance to facilitating cultural shows of developing environmental systems for pollution control.
3. Phonoaudiology—CSD professional education in Brazil
Out of approximately 48,000
The Ministry of Education determines education guidelines for phonoaudiologists that guarantee basic standards for the whole country. The guidelines allow different programs address specific needs and characteristics associated with different regions, cultures, and institutions. The number of programs in the different regions of Brazil is roughly associated with the size of the population therein, as can be observed in Figure 4. Programs include a minimum of 800 h of supervised practice in clinical schools and school hospitals, with supervision by professors [6]. These services are offered free of charge. They include populations that are usually underserved in all the regions of the country.
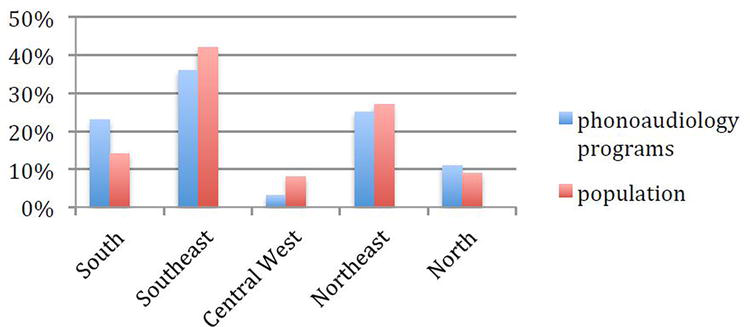
Figure 4.
Distribution of Phonoaudiology bachelor programs and of the population in the different regions of Brazil.
The first programs were developed in Brazil in the 1950s decade. One of them was part of the education department of a catholic university and the other was part of the otorhinolaryngology department of a school of Medicine. As expected, there are clear differences regarding how each program approaches cultural competence in professional education. In both programs, as is the case in all Phonoaudiology education, the opportunities for supervised practice involve contact with a very diverse population.
Cultural Competence refers to a continuously evolving process that involves self-awareness regarding our actions with individuals from cultures that are different from our own. It includes considering the culture, beliefs and values of students, clients and patients in any decision-making and intervention processes.
Therefore, fostering competencies of cultural awareness, respect and empathy is part of the supervisors’ routine work. However, there is not a uniform approach to this content by the different programs; there is a constant search for improvement, based on specific institutional aims and policies.
For example, in one of the oldest programs mentioned above, 5 years ago, after ample discussions by the faculty, a new educational project was approved. According to the project, students started observing supervised practice during the first semester of the program. This activity enabled the early start of discussions about cultural diversity and exercises of cultural competence. These experiences continue to develop, involving different activities and experiences in all the 10 semesters of the program, with effective practice in various scenarios in the last four semesters.
Regarding reach-out projects, depending on the specific pedagogical plan of each program, before the COVID-19 pandemic, actions from various programs focused on cultural diversity in different contexts. They involved, for example, screening for hearing and communication disorders in regular visits to riverside communities in the Amazon region by students from the state of Sao Paulo. Other groups could be involved in programs developed in small towns in the Southeast region, or reaching refugees that arrived from countries such as Venezuela, Haiti, or Colombia.
Cultural competence has been part of the different programs, with different intensities and approaches, for several years. There is not a specific policy about it, determining how or at which moment of the program the issue should be addressed. Therefore, each program can place the focus on cultural competence according to the specific academic context.
The process of getting access to academic education in Brazil is a process mostly based on the results of specific academic exams. Therefore, usually, the groups of students are also comprised of individuals from different social, economic, and cultural backgrounds. Dealing with these differences is an important issue in academic programs, and most important in areas that deal with human communication and interaction, such as Phonoaudiology.
4. Changes and challenges presented by the COVID-19 pandemic
Brazil has public systems that guarantee integral health care and 9 years of fundamental education to the whole population. However, these systems do not eliminate the severe inequities that can be observed everywhere. The COVID-19 pandemic had a major impact in several areas of health care delivery. Despite a vaccination system that otherwise works very efficiently and a population that was willing to be vaccinated, the distribution of vaccines was delayed and the process was very slow. The health system collapsed in all regions of the country, with overloaded ICUs and even a shortage of oxygen at some moments.
As occurred in several countries, the Brazilian central government was slow to respond to those challenges, failing to provide leadership aimed toward unified and collaborative actions. All decisions were transferred to state and city authorities, resulting in disjointed efforts and few positive results.
More than 650,000 persons perished, millions were infected, and continue to struggle with the consequences. Economic impacts continue to be observed in unemployment, increasing numbers of bankruptcies, hunger, and homelessness. These consequences are evident in all regions and affect either rural or urban populations.
Now, more than 1 year after the start of the vaccination in Brazil, a significant proportion of the population is vaccinated and the number of infections and deaths are decreasing. Several restrictions are being suspended, face-to-face activities are starting, and schools are re-opening. However, the consequences of the COVID19 pandemic will probably continue to affect the educational, health, and economic systems for a long time. It is not possible to think that things will be “back to normal” within a short period. It is important to think, for example, not just about children that were sick with COVID-19 and the long-term consequences of long hospitalization periods with, eventually, reduced oxygen amounts provided to the brain. Health, educational, and social security systems will have to deal with a great number of children that were orphaned and how to guarantee equal chances and compensating intervention. There are several challenges that will have to be met in the near and farther future.
4.1 Phonoaudiology education and the pandemic
Since the onset of the pandemic, in the first semester of 2020, it became clear that social distancing was one of the most effective ways of avoiding the spread of the COVID-19 pandemic. Authorities and stakeholders proposed several strategies to reduce human physical contact while trying to maintain most of the activities we used to consider “normal.” Most of the universities either enhanced or implemented online classes, study groups, and supervisions. However, it was believed that this situation would last for a few weeks or a few months at the most. During those first weeks, there was a somewhat relaxed approach to the new challenges with expectations such as “
As a result, different groups proposed and organized different responses. Some universities interrupted completely their activities, while others continued with online theoretical courses but interrupted all practice. Still, others built on previous experience and expertise in telehealth in order to continue to offer services. This also facilitated the establishment of clinical competence for future practice.
Telehealth or telepractice is the use of digital information and communication technologies, such as computers and mobile devices, to access and provide/receive health care services remotely.
Access to the Internet and digital equipment varies widely among students. In some cases the public university provided equipment and Internet packages to students, aiming to improve equity of access to tele-practice, tele-supervision, and distance education among students. The same was not true for many patients. It was not as easy to reduce the differences between patients from different social and cultural backgrounds, who did not have access to such technologies. Barriers to providing services through remote technologies also included the parent’s education level, their proficiency in the use of digital technology, and involvement with the intervention process.
Remote technologies can include, personal computers, notebooks, tablets and mobile phones.
As weeks, months and a year went by it became clear that those who started adapting their practices earlier had more effective results and better outcomes. This applied to teaching activities involved in theoretical courses as well as interventions associated with supervised practice.
The COVID 19 pandemic made even more evident another unwanted kind of social distancing. Differences in access to basic health resources highlighted social differences. As a result, discussions with students about alternatives to address the various and specific difficulties became frequent topics of classes and supervision meetings. Through such discussions, access to technology emerged as another challenge to be addressed in the process of increasing the equality of chances and opportunities for all.
Even considering that there are an increasing number of Internet users, there is still a large proportion of the population without any access to the web. Concerns about the use of digital technology in school environments, which have yielded poor results despite some public policies supporting accessibility to persons with special needs, are reported [7].
Research conducted before the pandemic revealed that, with 71% of the Brazilian population responding, 28% of the households did not have access to the Internet; 25% of the population did not use the Web and only one-third of the participants did any kind of work through the Internet. People living in the rural area (79%) or with lower income (85%) reported using the Internet exclusively on their cell phones [8].
A study focused on children and adolescents before the pandemic informed that there were 3 million children and adolescents that did not have access to the Internet in Brazil; of which 1.4 million never had access to the Web either in school, at work, or at home. Besides that, 4.8 million children and adolescents between 9 and 17 years (18% of the population) did not have access to the Internet at home [9]. Considering the use of digital technology in the schools, the study reports that 58% of the students from urban schools used cell phones to perform school activities and only 33% of the teachers had some kind of instruction about the use of the Internet. In rural environments, only 40% of the schools had at least one computer with access to the Internet and 9% could access the Web via other devices [10].
Telehealth resources have great potential to address barriers such as the lack of professional experts in a specific area, and physical distance, besides saving transportation time and costs. However, not all families have access to the best technology devices to allow for the best services of online therapy. Professional education programs should include competencies regarding the resources available in different contexts.
It seems that the alternative strategies that had to be used in the implementation of tele-practice represent an important experience to be considered in offering SLP services to underserved or unserved populations and to in-training professionals that will be able to use them [11]. A study [12] conducted in 2020 assessed the reactions of final-period undergraduate students after 10 weeks of supervised telepractice with children with ASD in Sao Paulo, Brazil. Results indicate that 70% of them reported being self-confident and encouraged and that it was possible to continue the learning process. They considered that the improved contact with the families was the most positive aspect of telepractice, while the negative aspects were the lack of personal contact and the dependency on technology. This same publication [12] reports on 552 sessions of online language therapy with 83 children with ASD. These data highlight the importance of flexibility in the use of the available technology. More than 50% of the contacts occurred through WhatsApp. This surely is not the best way to provide a speech-language therapy session, but the alternative was no therapy. Overall, in 76.3% of the sessions, the therapists (supervised students) reported that the specific goals were met. These preliminary results seem to indicate that even in a situation where the resources are not the best ones, telehealth seems to be a viable alternative to the delivery of SLP services to children with ASD and their families.
5. Cultural awareness and cultural competence
Cultural differences and characteristics are not just observed in the minorities represented by migrants, refugees, and persons that frequently lack adequate access to basic housing, health, and education services [11]. They can also be observed in everyday life in small attitudes, and in regional popular sayings and customs that involve social, cultural, and economic aspects. Critical thinking is necessary to understand cultural differences that may reflect power differences associated with cultural identity. The notion of cultural humility [13] involves a better understanding of health issues regarding the context in which they occur.
Cultural awareness is essential to all SLPs in everyday situations [14], but more so when the service is provided through technological resources that “put the therapist inside the client’s home.”
This is the situation either when the therapist proposes to work with the client with the assistance of an adult at home or if “guiding” activities that are to be conducted at home by a familiar adult. Anyway, we are “invading” the client’s home (and probably the whole family), by being part of the routine of other family members, sharing routines and habits. Regardless of how productive it can be for the work itself, allowing the inclusion of tasks and abilities in the child’s routine and environment, we are entering their homes and it is easy to consider that this “participation” maybe a little (or too much) more than the families anticipated. The same may be true about online teaching. The study setting for the student may not be appropriate; or the student may feel uncomfortable and exposed, sharing their home environment or a disrupted routine during a class or supervision. It can happen anywhere, with anyone. Building the notion that improving cultural competence will be a never-ending task for any professional that deals with people, education, or communication should be part of the aims of education regarding remote access in education and intervention for the future.
The pandemic interrupted projects of modernity previously proposed and the need for changes has emerged. The ruptures created by the pandemic may represent an important opportunity for society to overcome barriers imposed by prejudices, lack of coherent information, and other elements that can harm the action of the speech therapist within the clinical practice. The notion of telepractice as the only mode of access between the phonoaudiologist and the client/patient during a long period and the cultural aspects involved has never been discussed like this before. Cultural competence in remote practice is now an essential part of the equation.
The concept of cultural competence has already been studied by several specialties within the area of health, addressing how it can benefit both the professional and the patient. One of the studies highlights that culture is not only something that people have but also something present in every human being, in its roots, which influences all their actions. In the literature, cultural aspects have already been defined as a set of values, beliefs, and norms that guide the thinking and decision-making processes of a certain population group about the actions it takes [15, 16]. Then, if the culture in which individuals are born can determine the thought and actions of each individual and the group, the expansion of this culture and the encounter, clash, and confluence with other cultures, can modify complete mental processes as well as personal, professional, and group decision-making mechanisms [17].
The phonoaudiologist is the professional trained to assist the language and communication skills of individuals of all ages. The assistance, however, should consider all complex issues regarding cultural sensitivity in all aspects involved in the integration of knowledge, competencies, and attitudes that influence therapeutic practice. Betancourt et al. [18] pointed out that the health professionals’ awareness of these complex dimensions that relate to cultural competence incorporates the understanding of the influence of social and cultural issues on beliefs and behaviors, taking into account their interaction with health providers. For these reasons, the COVID-19 pandemic and the need to transform all intervention, supervision, and education activities to remote access, made it clear that cultural competence must include these resources as part of the discussions during the speech-language pathologist’s training.
The understanding of the multicultural aspects of clients with speech, language, and hearing problems is essential to the professional’s ability to perform their best practices, providing a high-quality service for the population.
A small study conducted online interviews with 54 undergraduate and graduate students of Phonoaudiology and questioned their positions on the relevance of cultural competence in their professional training and their ability to work with individuals from different cultures. The results indicate that only 20% of the participants considered they had good knowledge about different cultures and 70% would be interested in different cultural experiences. This is important feedback regarding teaching strategies. Faculty needs to address how to bring cultural awareness as one of the competencies that are focused in several academic activities so students would be able to recognize and value the experiences they are already having with persons from different cultures. Different strategies may be used to achieve this goal, such as lectures, online discussions, or classroom activities [19]. The challenges imposed by the pandemic, restricting personal contact, will demand the continuity of the search for the best strategies.
6. Considerations
The small study reported above confirms the expectations of Brazilian students in the area of communication sciences and disorders regarding the impact of experiences with different cultural groups on the development of cultural competence. The limitations imposed by the COVID-19 pandemic delayed all planning about face-to-face contact in the short term. However, there are many alternatives for distance meetings and communication. Developing communication partnerships among students and universities from different regions, environments, and even countries can foster interaction between students and improve general cultural sensitivity. Hopefully, the return to more mobile possibilities will allow the continuity and improvement of previous experiences.
Even different languages should not be barriers if communication is the true aim. Learning how to understand each other and reducing differences and distances may be the kind of soft skill that contributes to the development of empathy. It can surely be interesting for a CSD student to experience the role of not being able to communicate efficiently and needing to overcome linguistic and cultural barriers and becoming more flexible in different settings. It may be said that empathy is not enough, but it can be an important intrinsic motivator to the development of cultural competence.
References
- 1.
Holanda SB. Roots of Brazil. Notre Dame, Indiana, United States: University of Notre Dame Press; 2012. (First published in 1936) - 2.
Portal da Imigração. 2021. Available from: https://portaldeimigracao.mj.gov.br/images/dados/relatorio-anual/2020/Resumo%20Executivo%20_Relat%C3%B3rio%20Anual.pdf - 3.
Ribeiro D, Ribeiro GL. The Brazilian People: The Formation and Meaning of Brazil. Florida: University Press of Florida; 2000 - 4.
Freyre G. The Masters and the Slaves—A Study in the Development of Brazilian Civilization. California: University of California Press; 1986 - 5.
Survival Brasil. 2021. Available from: https://www.survivalbrasil.org/povos/indios-brasileiros - 6.
Fernandes FDM, Wertzner HF. Competence-based curricula for the education of speech-language pathologists and audiologists in Brazil. Folia Phoniatrica et Logopaedica. 2014; 66 (4–5):176-182. DOI: 10.1159/000366129 - 7.
United Nations Education, Science and Culture Organization. Assessing Internet Development in Brazil: Using UNESCO’s Internet Universality ROAM-X Indicators NIC.BR/CETIC.BR. 2019. Available from: https://cetic.br/publicacao/assessing-internet-development-in-brazil-usingunesco-s-internet-universality-roam-x-indicators/ - 8.
Centro Regional de Estudos para o Desenvolvimento da Sociedade da Informação. Survey on the Use of Information and Communication Technologies in Brazilian Households: ICT Households. 2018. Available from: https://www.cetic.br/publicacao/pesquisa-sobre-o-uso-das-tecnologias-de-informacao-e-comunicacao-nos-domicilios-brasileiros-tic-domicilios-2018/ - 9.
Centro Regional de Estudos para o Desenvolvimento da Sociedade da Informação. Survey on Internet Use by Children in Brazil: ICT Kids Online Brazil São Paulo. 2017. Available from: https://cetic.br/publicacao/pesquisa-sobre-o-uso-da-internet-por-criancas-e-adolescentesno-brasil-tic-kids-online-brasil-2017/ - 10.
Centro Regional de Estudos para o Desenvolvimento da Sociedade da Informação. Survey on the Use of Information and Communication Technologies in Brazilian Schools: ICT in Education. 2017. Available from: https://cetic.br/publicacao/pesquisa-sobre-o-uso-das-tecnologias-de-nformacao-e-comunicacao-nas-escolas-brasileiras-tic-educacao-2017/ - 11.
Levey S, Moonsamy S. Unserved and Underserved Populations: New Approaches to Inclusivity. New York: Peter Lang Publisher; 2021 - 12.
Fernandes FDM, Sun IYI, Rodrigues BF, Cabral CP, Tosetto C, Segeren L. Speech language therapy for children with ASD and their families during the Covid-19 pandemic: Considerations about professional training and service delivery on a majority country. Highlights on Medicine and Medical Research. 2021; 4 :32-38. DOI: 10.9734/bpi/hmmr/v4/7594D - 13.
Greene-Moton E, Minkler M. Cultural competence or cultural humility? Moving beyond the debate. Health Promotion Practice. 2020; 21 (1):142-145. DOI: 10.1177/1524839919884912 - 14.
Hyter YD, Salas-Provance MB. Culturally Responsive Practices in Speech, Language, and Hearing Sciences. San Diego, California: Plural Publishing; 2018 - 15.
Leininger MM, McFarland MR. Culture Care Diversity and Universality: A Worldwide Nursing Theory. Burlington, Massachusetts, United States: Jones & Bartlett Learning; 2006 - 16.
Luquis RR, Pérez MA. Cultural Competence in Health Education and Health Promotion. Hoboken, New Jersey, United States: John Wiley & Sons; 2021 - 17.
Clauss-Ehlers CS, Sood AB, Weist MD. Introduction: An urgent call to understand the status of children and young people within a social justice paradigm. In: Clauss-Ehlers CS, Sood AB, Weist MD, editors. Social Justice for Children and Young People: International Perspectives. UK: Cambridge University Press; 2020. pp. 3-19 - 18.
Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O. Defining cultural competence: A practical framework for addressing racial/ethnic disparities in health and health care. Public Health Reports. 2003; 118 (4):293-302. DOI: 10.1093/phr/118.4.293 - 19.
Chae D, Kim J, Kim S, Lee J, Park S. Effectiveness of cultural competence educational interventions on health professionals and patient outcomes: A systematic review. Japan Journal of Nursing Science. 2020; 17 (3):e12326. DOI: 10.1111/jjns.12326