
Abstract
The impact of COVID-19 is significant in the body system, one of which is the central nervous system (CNS) involved in controlling all aspects of human behavior and coordination. This shows the need to assess from various studies in human and animal models the neurological effects of this virus. Some of the reported effects include loss of taste and smell, headaches, delirium, dizziness, ischemic stroke, and brain inflammation. It is essential to review the acute, chronic or transient neurological effects. This will enhance and/or improve treatment designs and management modalities for the COVID-19. We critically revise the literature and contribute to the body of knowledge in this line of research. Here in this chapter, we highlighted the various neurological disorders caused by COVID-19 and examined the relationship between the neurological systems and COVID-19. As well as evaluate current treatment/management modalities including vaccines and prospects for the future.
Keywords
- COVID-19
- SARS-CoV-2
- neurological disorders
- neurological symptoms
- treatment/management modalities
1. Introduction
COVID-19 causative virus (SARS-CoV-2) affects many body organs and systems to induce its pathogenesis. The disease is severe in people with comorbidities such as obesity, diabetes, hypertension, chronic respiratory disease, cerebrovascular disease, and chronic kidney and liver disease [1].
In neural tissues, the mechanism of invasion is well-established. It involves the interaction of ACE2 (Angiotensin-converting enzyme 2) receptors and spike protein. SARS-CoV-2 enters the nervous system via neurotropism, hematological dissemination, vasculotropism, and cytokine storm [2, 3].
Some of the common neurological symptoms of SARS-CoV-2 include CNS symptoms; (dizziness, delirium, confusion, prominent agitation, and dizziness), acute cerebrovascular disease, and epilepsy; PNS symptoms; ageusia (loss of sense of taste), hypogeusia (reduction in the ability to taste), anosmia (inability to smell), hyposmia (reduction in the ability to smell), and neuralgia (painful sensation in the body) and skeletal muscular symptoms: myalgia/fatigue and muscle injury [3, 4].
Many bioactive compounds have been reviewed for their antiviral effects which may have both preventive and curative effects [5]. Mainstay pharmacological/non-pharmacological interventions for prevention, management, and treatment include COVID-19 vaccines, remdesivir [6], SARS-CoV-2 targeting monoclonal antibodies such as Casirivimab and Imdevimab, Immune modulators (Baricitinib), immunosuppressive therapy as well adherence to public health guidelines such as handwashing, use of alcohol gels and face masks, etc.
In this chapter, we highlighted various neurological disorders and symptoms caused by COVID-19 and examined the relationship between the neurological systems and COVID-19. Additionally, we evaluated current therapies including the administration of vaccines, anti-virals, and their prospects for future applications.
2. COVID-19
The novel coronavirus disease (COVID-19) has been a dire threat to public health, the global economy, and human co-existence since its first report in Wuhan, China in 2019 [7]. Globally, as of 2nd June 2022, there have been 6,293,414 deaths due to COVID-19 out of 528,275,339 confirmed cases. To curtail the menace of COVID-19, 11,947,644,522 vaccine doses have been reported administered globally [8]. Prior to the development and administration of vaccines, a number of preventive measures (hand-washing under running water, use of alcohol-based hand sanitizer, social distancing, wearing of face mask, etc.) were put in place by health regulatory bodies to manage the transmission of the disease [7]. These measures were evaluated to study compliance and effectiveness in curbing the spread of the virus [9, 10, 11]. Although the global incidence and mortality rate has declined, adherence to preventive measures and vaccination is still encouraged.
COVID-19 severity has been reported in elderly patients and those with comorbidities (obesity, diabetes, hypertension, chronic respiratory disease, cardiovascular disease, cerebrovascular disease, chronic kidney, and liver disease) [1, 12]. Due to the novelty of the disease, the possibility of other long-term effects is still unknown. However, those with severe cases of infection can develop acute or chronic effects (graphical abstract) such as chronic fatigue syndrome, complications of the heart, lung, and kidney, neurological defects (loss of taste and smell, delirium, headaches, brain inflammation, stroke, and Guillain-Barre syndrome) [12, 13]. This calls for a need for closer monitoring and more research into the aftermath effect of the COVID-19, even in well-managed patients.
3. Mechanism of neurological pathology
The SARS-CoV-2 respiratory indices are well known and reported. Recently, there has been a significant increase in evidence showing anosmia (complete loss of smell) as a SARS-CoV-2 symptom, indicating a high level of neurological involvement following the infection and also SARS-CoV-2 having neuro-invasive properties. Studies suggest that SARS-CoV-2 enters the central nervous system (CNS) in either of the two ways; through systemic vascular dissemination or across the cribriform plate of the ethmoid bone, which might have consequences concerning anosmia as experienced by the SARS-CoV-2 patients [14]. The virus invades the neural tissue once in the systemic circulation due to its neurotropism properties and then, binds and interacts with ACE2 (Angiotensin-converting enzyme 2) receptors in the endothelium capillary via the spike proteins [14, 15]. Previously, ACE2 has been shown to be expressed in the upper and lower epithelium of the airways together with the CNS endothelial capillary [16]. One of the studies conducted evaluating SARS-CoV-2 spike glycoprotein structural integrity showed an approximately 20- a fold affinity increases to ACE2 when compared to the spike protein of the sister virus SARS-CoV-2 [17]. However, using BLASTp, the spike proteins of the two sister viruses are structurally similar but not identical, explaining the differences in the neurological prevalence. Meanwhile, not all the human cell lines that express ACE2 are susceptible to the novel coronavirus infection. Nevertheless, several neurological manifestations of the SARS-CoV-2 infection should be given absolute attention together with its well-understood respiratory index.
3.1 Stroke
Stroke is now common, developing, and/or potentially devastating SARS-CoV-2 infection complication [18]; about 2–6% of hospitalized COVID-19 patients have developed an acute cerebrovascular event [19]. In 2020, a large vessel stroke was reported in five patients (< 50 years of age) infected with SARS-CoV-2 [20]. Studies on the thromboembolic complications rate in SARS-CoV-2 patients showed 1.6% [21] and 2.5% [22] reported ischemic stroke occurrences. Klok and Lodigiani showed that the thrombotic complications were significantly high for their respective institutions. However, there are other risk factors predisposing COVID-19 patients to thromboembolic stroke development beyond the usual metabolic and cardiovascular co-morbidities. At this moment, various mechanisms of SARS-CoV-2 induced stroke have been reported including myocardial damage with cerebral embolism, coagulopathy, or pre-existing atheroma plaque destabilization [23]. The viral invasion led to thrombosis by activating immune response involving platelets, endothelium, and coagulation. Furthermore, SARS-CoV-2 causes cytokine storms resulting in increased D-dimers, affecting coagulation, and inducing stroke. Also, viral invasion can lead to heart damage, resulting in viral myocarditis and finally cardioembolic stroke. Inflammation can destabilize the fibrous capsule surrounding the atheroma plaque, eventually, exposing the thrombogenic clotting material, initiating arteries clogging and thus, causing a stroke [23].
3.2 Guillain-Barré syndrome (GBS)
GBS is an acute acquired autoimmune disorder of the peripheral nerves that occurs as a result of infection [24]. Actually, GBS is symmetrical ascending paralysis, mostly due to bacteria or viral infection of the respiratory or gastrointestinal tract [25]. It is a rare disease of the peripheral nervous system (PNS) with approximately 1.11 in 100,000 incidences annually [26]. Since the COVID-19 outbreak, the number of GBS cases has increased significantly. There have been some confirmed cases and a potential report of GBS as significant SARS-CoV-2 neurological sequelae. Among the eleven cases published in the literature, there is substantial capriciousness in an indication of GBS onset, together with distinctive respiratory distress of SARS-CoV-2 [27]. GBS is related to recent inoculation from a possible range of pathogens, explaining the disease’s clinical heterogeneity [28]. Despite the inconsistency in the symptom onset in relation to COVID-19 diagnosis, it is of note that most reports described constant clinical features of variable sensory abnormalities with deep tendon reflex loss and lower limb weakness over the upper limb. Various mechanisms the virus uses to trigger acute areflexic state in GBS have been reported. Possibly, antibodies against the surface glycoproteins are generated against the pathogen which also responds to the comparable native protein structures located on the neuronal surface leading to GBS clinical features [29]. Another probable mechanism is the macrophage activation syndrome (cytokine storm) and hyper-inflammation might be involved in GBS pathogenesis in SARS-CoV-2 individuals [30].
3.3 Neurocognitive disorder
Individuals with neurocognitive disorders have a high risk of being infected with COVID-19. APOE e4 increases the risk of Alzheimer’s neurocognitive disorder. Previous studies revealed that the deformed blood–brain barrier (BBB) in Alzheimer’s patients predisposes them to infections. Furthermore, memory impairment related to neurocognitive disorders could possibly affect the patient’s capability to observe the COVID-19 preventive measures including the use of masks, hand-sanitizing, and social distancing [31]. Individuals with neurocognitive disorders are more liable to experience comorbidities including diabetes, pneumonia, or cardiovascular disease increasing their risk of severe morbidities or death if they contract COVID-19 [32]. Previous research has found a bidirectional association between viral infections and neurocognitive disorders. Patients with neurocognitive disorders have a higher chance of viral infection and patients with a poor immune response to the infection have a higher risk of neurocognitive disorders [31]. Further research is needed to understand if the molecular and socioeconomic interactions play role in the higher incidence of COVID-19 in patients with neurocognitive disorders patients, and to identify whether SARS-CoV-2 infection accelerates or triggers neurocognitive disorders [31].
3.4 Movement disorders
COVID-19 could potentially aggravate neurological symptoms in PD individuals [33]. The effect of COVID-19 on individuals with Parkinson’s (PD) disease is multifaceted as SARS-CoV-2 can affect their health directly, with a downstream effect on the advancement of the disease and the quality of life. Several studies have reported the onset of deteriorating PD and motor symptoms (for example speech disturbance, fall, dystonic spasms) preceding COVID-19 diagnosis [34, 35, 36]. Motor symptom changes might be a result of a decrease in oral therapy absorption due to diarrhea -a COVID-19 symptom [37]. Worsening of the symptoms can be ascribed to the pandemic subordinate effects including changes in normal activities and stress. Fatigue, rigidity, pain, concentration, and tremor were recorded during neurological symptoms evaluation for individuals with PD a month before the pandemic began and beyond [38].
3.5 Hypoxia
Several COVID-19 patients appeared to have severely low blood oxygen saturation levels [39], leading to hypoxia which causes damage to the tissues [40]. Meanwhile, these patients do not get enough oxygenation via the blood, COVID-19 individuals with hypoxia often do not show much respiratory distress, but they feel alert, and can easily talk [39]. Hence, hypoxia in COVID-19 individuals is often known as “happy” or “silent” hypoxia due to its minimal additional effects [39]. In a study by Mortaz et al. COVID-19 participants’ RBC had higher amounts of intracellular NO (nitric oxide). This is not due to hypoxia per se, but it could provide protection against the hypoxia reported in COVID-19 patients. Constitutive NO generation in RBCs is mostly dependent on NOS during health, although NO production in hypoxic settings may entail nitrite reduction by deoxyhemoglobin carbonic anhydrase and/or eNOS itself. Also, COVID-19 participants’ RBC had higher amounts of intracellular NO [39].
4. Relationship and effects of COVID-19 on neurological systems
In the past, viruses such as arbovirus, measles virus, enterovirus, herpes simplex virus (HSV), Varicella-Zoster virus (VZV), Cytomegalovirus (CMV), Epstein -Barr virus (EBV), and Human JC virus (JCV) have been reported to invade the nervous systems of hosts with severe neurological effects [41]. Now, SARS CoV-2 (severe acute respiratory syndrome coronavirus 2), the virus that causes COVID-19 has joined that list with recently reported neurological manifestations of the disease. The mode of entry of these viruses including SARS CoV-2 has been thoroughly studied and classified into the several major routes: endocytosis (direct fusion with neurons), sensory nerve endings, synapses, and axons, circulating leukocytes, lymph nodes, the blood–brain barrier (BBB), the Central Nervous System (CNS) and the Peripheral Nervous System (PNS) [42].
4.1 SARS-CoV-2 and angiotensin-converting enzyme 2 (ACE2)
ACE2 has a high affinity for SARS-CoV-2 (Figures 1 and 2). SARS-CoV-2 interacts with ACE2 receptors to invade the cells in the body [45, 46] by receiving the spike (peplomer) glycoprotein of the virus. mRNA expression profile of ACE2 shows that the enzyme is organ-specific but expressed in almost every tissue in the body [46, 47]. ACE2 receptor is usually found in the pulmonary type II alveolar cells and respiratory epithelial at high levels because COVID-19 is primarily a respiratory disease [48, 49]. ACE2 is also found in other body tissues and cells such as myocardial and endothelial cells [50], kidney, stomach, colon, and ileum cells [51], oral mucosa cells [52], astrocytes, neuron and glial cells of the brain and spinal cord tissues (Figure 1) [14].
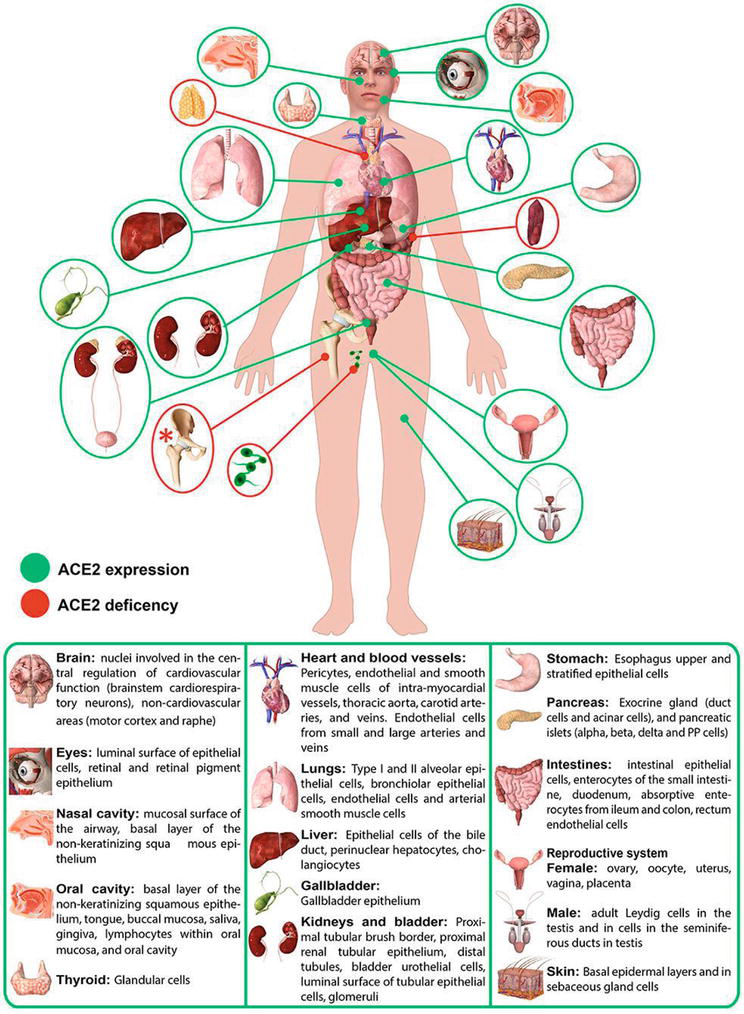
Figure 1.
Distribution of ACE 2 in the human body. (image adapted from [
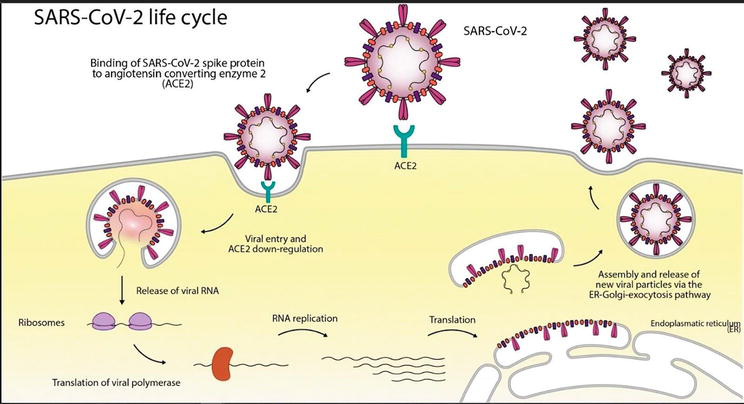
Figure 2.
SARS-CoV life cycle (image adapted from [
The ACE2 gene is located on chromosome Xp22.22 and contains 18 exons and 20 introns [53]. It produces an 805 amino acid, type I transmembrane glycoprotein which contains a 17-amino-acid N-terminal signal peptide and a 22-amino acid C-terminal membrane hydrophobic transmembrane region anchoring it in the cell membrane [46]. It also has a HEXXH zinc-binding metalloprotease motif, a C-terminal collecting domain, and an insulin-like domain [53]. ACE2 gene expression is also found in other respiratory disorders such as SARS, Middle East respiratory syndrome (MERS), and H1N1 influenza [54].
4.2 Relationship of COVID-19 with neurological systems
SARS-CoV-2 directly attacks neural cells and infects cerebrovascular endothelium and brain parenchyma (medial temporal lobe) causing early apoptosis and necrosis (Figure 3) [4, 44, 48]. This attack occurs through a series of mechanisms such as proteolysis, viral fusion with membrane, and entry mediated by ACE2 and transmembrane serine protease 2 (TMPRSS2) in some parts of the brain, CNS, PNS, and cerebrospinal fluid described through animal studies [see 55, 56, 57, 58 for more details].
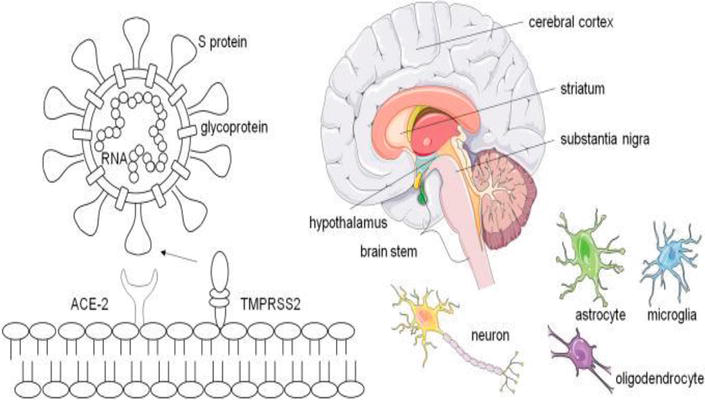
Figure 3.
Neurotropism of SARS-CoV-2. SARS-CoV-2 (image and description text and Servier medical art,
4.3 Proposed mechanisms of coronavirus entry into the nervous system
Neurotropism: retrograde transfer from the olfactory epithelium to the brain via cribriform plate (Figure 4) [3, 49].Hematological Dissemination: damage to the blood–brain barrier during the viremia phase [3, 14]. Brain areas devoid of a blood–brain barrier such as the circumventricular organs are particularly vulnerable to circulating inflammatory mediators.Vasculotropism: Transfer from peripheral nerve terminal to CNS via synapse connected route [4, 13].Cytokine Storm: increase in cytokine serum levels [4].
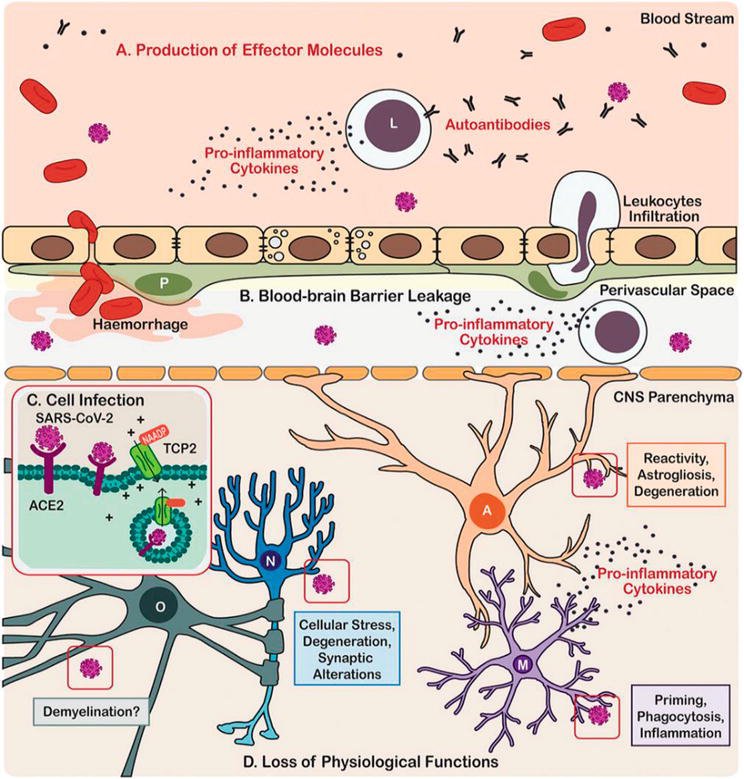
Figure 4.
Scheme illustration of the neurotropism, neuroinflammatory processes, and effects on brain cells triggered by COVID-19 in patients. Image and description text adapted from [
Spike (S) proteins bind the angiotensin-converting enzyme 2 (ACE-2) receptor of the target cell. Cleavage of the S protein by type II transmembrane serine protease (TMPRSS2), facilitates viral entry. ACE-2 mRNA expression and double-positive ACE-2 + TMPRSS2 + cells have been identified, among others, on neurons and glial cells, in the cerebral cortex, striatum, hypothalamus, substantia nigra, and brain stem, making the CNS potential direct targets of SARS-CoV-2 infection.
Immune cells from the periphery and the central nervous system (CNS) (A) Produce effector molecules that include pro-inflammatory cytokines and autoantibodies. (B) SARS-CoV-2 infection also causes leakage of the blood–brain barrier leading in some cases to hemorrhage and cerebral infarct, as well as eliciting leukocyte infiltration. (C) In the parenchyma, the CNS cells become infected by SARS-CoV via angiotensin-converting enzyme 2 (ACE2) endocytosis mediated by the two-pore channel 2 (TCP2). (D) SARS-CoV-2 infection leads to loss of physiological functions of the brain cells, including neurons, astrocytes, microglia, and oligodendrocytes. Cell types are identified in the following manner; A, Astrocyte; L, Leukocyte; M, Microglia; N, Neurone; O, Oligodendrocyte.
4.4 Effects of COVID-19 on neurological systems
Several case reports of SARS-CoV-2 from hospitals, clinical settings, and study groups indicate different manifestations of neurological symptoms and effects [43, 60]. These studies report these common neurological manifestations to occur in the brain, olfactory areas, and central nervous system. A report from the treatment of a COVID-19 patient carried out by [61] described encephalitis (inflammation of the brain) detected through CT scans as a clinical manifestation of SARS-CoV-2 infection. One study in China. Another study in the UK reported that patients developed unexplained encephalopathic features (detected through MRI) and showed a cognitive decline [62]. Additionally, an autopsy of human brain samples from neurologically diseased patients showed the presence of the virus in the cortical neurons of the brain [55, 63]. This presence is attributed to inter-neuronal propagation and axonal transport of the virus into the CNS. These reports constitute evidence that SARS-CoV-2 has neuro-invasive potential. It also stresses the need for further research to ascertain the level of damage it can cause in neurological systems as the exact mechanism of invasion is still unclear.
4.5 Neurological symptoms are classified into three categories
CNS symptoms or diseases: headache, ataxia, corticospinal tract signs, impaired consciousness (confusion, prominent agitation, and dizziness), acute cerebrovascular disease, and epilepsy [2, 3, 14, 59, 64].PNS symptoms : ageusia (loss of sense of taste), hypogeusia (reduction in the ability to taste), anosmia (inability to smell), hyposmia (reduction in the ability to smell), and neuralgia (painful sensation in the body).Skeletal muscular symptoms : myalgia/fatigue and muscle injury.
Similarly, clinical manifestations such as stroke, acute necrotizing hemorrhagic encephalopathy, acute Guillain–Barré syndrome, and meningitis usually accompany the neurological effects of COVID-19. But they are frequent in individuals who are critically ill, adults who are old, and people who have suffered from previous infections of embolism or cardiovascular diseases [20, 65, 66].
5. Possible therapies for COVID-19
Numerous probable therapies for COVID-19 are being studied and tested, but, fortuitously, some medications have been approved by the FDA and made available for infected individuals [6]. Some pharmaceutical medications are being evaluated as possible therapies with different degrees of success [67]. Hydroxychloroquine, an antimalarial and anti-inflammatory drug, was first suggested to have potential against COVID-19 [6], but was later shown to be ineffective [68]; Ribavirin inhibits viral fusion and entry into host cells [6]. The use of Remdesivir for COVID-19 treatment prevented SARS-CoV-2 replication, while tocilizumab, an antagonist drug, also prevents the virus entry into the host cells [6].
ATN-161 has been shown to affect as an anti-cancer and ischemic stroke agent and has successfully completed phase I clinical trial for cancer showing to be well-tolerated without any toxicity. In an ischemic stroke study, increased expression of α5β1 integrin in post-stroke brain endothelial cells was linked to BB breakdown and then increased neuroinflammation and edema. These conditions can be inhibited by ATN-161 [71]. ATN-161 has been shown to be a potential antiviral therapy following a study that reported ATN-161 blocking viral replication of the beta-coronavirus porcine hemagglutinating encephalomyelitis virus (PHEV) in mice through the α5β1-FAK signaling mechanism [69]. In the study, it was found that SARS-CoV-2 spike protein was attached to α5β1 and α5β1/hACE2 which was inhibited by ATN-161 in VeroE6 cells in vitro. This study, therefore, recommends further studies on the ATN-161 as a possible COVID-19 therapy against COVID-19 related neurological disorders. The last possibility for a possible treatment is convalescent plasma, in which the infected individual receives plasma from a recovered COVID-19 individual. This was done in optimisms that the antibodies in the plasma of the improved individuals could help fight the virus in infected ones [67].
Managing prior neurological diseases such as stroke might remain similar to the pre-COVID-19 era. Continuing immunomodulation should continue as well as constant for drug-related adverse effects observation, since withdrawal may initiate a reversion [70]. Individuals involved must consciously observe hand hygiene and social distancing to avoid being infected with SARS CoV-2 [71, 72].
6. Conclusion
The COVID-19 pandemic has impacted our lives beyond health. Today, we have learned new ways of dealing with a pandemic and our understanding of viruses has expanded to newer dimensions. In this chapter, we reviewed the specific effects of COVID-19 on the neurological system and the various symptoms in the CNS, PNS, and skeletomuscular systems. Studies done so far emphasize the need for further research to ascertain the level of damage SARS-CoV-2 can cause in neurological systems as the exact mechanism of invasion remains unclear. Once clearly defined, existing drugs can be repurposed, new pharmacological interventions can be developed, and combination therapies can be designed to relieve neurological symptoms and the effects of SARS-CoV-2 on neurological systems.
References
- 1.
Zhou Y, Yang Q , Chi J, Dong B, Lv W, Shen L, et al. Comorbidities and the risk of severe or fatal outcomes associated with coronavirus disease 2019: A systematic review and meta-analysis. International Journal of Infectious Diseases. 2020; 99 :47-56. DOI: 10.1016/j.ijid.2020.07.029 - 2.
Altunisik E, Sayiner HS, Aksoz S, Cil E, Ozgenc G. Neurological symptoms in COVID-19 patients. Bratislavské Lekárske Listy. 2021; 122 (1):39-44. DOI: 10.4149/BLL_2021_004 - 3.
Haider A, Siddiqa A, Ali N, Dhallu M. COVID-19 and the brain: Acute encephalitis as a clinical manifestation. Cureus. 2020; 12 (10):e10784. DOI: 10.7759/cureus.10784 - 4.
Aghagoli G, Gallo Marin B, Katchur NJ, Chaves-Sell F, Asaad WF, Murphy SA. Neurological involvement in COVID-19 and potential mechanisms: A review. Neurocritical Care. 2021; 34 (3):1062-1071. DOI: 10.1007/s12028-020-01049-4 - 5.
Teibo J, Olorunfemi F, Ajayi J, Adewolu M. Frugal chemo-prophylaxis against COVID19: Possible preventive benefits for the populace. International Journal Advanced Research in Biological Sciences. 2020; 7 :44-64 - 6.
Jean SS, Lee PI, Hsueh PR. Treatment options for COVID-19: The reality and challenges. Journal of Microbiology, Immunology, and Infection. 2020; 53 (3):436-443 - 7.
Omotoso OE. Contributory role of SARS-CoV-2 genomic variations and life expectancy in COVID-19 transmission and low fatality rate in Africa. Egyptian Journal of Medical Human Genetics. 2020; 21 :72. DOI: 10.1186/s43042-020-00116-x - 8.
WHO, 2022 Available from: https://covid19.who.int/ - 9.
Omotoso OE, Awoyemi P-P, Wahab VJ, Ragab M, Teibo JO, Akinfe O, et al. Knowledge and level of adherence to COVID-19 preventive measures: A Bi-national web-based survey in Africa December. Saudi Journal of Health Sciences. 2021; 10 :80-87 - 10.
Teibo JO, Teibo TKA, Omotoso OE, Olagunju AS, Omotoso E. A Bi-continental review of the knowledge and adherence to COVID-19 public health guidelines in north and South America. Infectious Diseases and Tropical Medicine. 2021; 7 :e728 - 11.
Omotoso OE, Omotoso EF, Paimo KO, Teibo JO, Olagunju AO. Knowledge and adherence to COVID-19 preventive measures: A continental review. Sudan Journal of Medical Sciences. 2021b; 16 (3):371-385 - 12.
https://www.nih.gov/news-events/news-releases/researchers-highlight-covid-19-neurological-symptoms-need-rigorous-studies#:~:text=Neurological%20symptoms%20that%20have%20been ,%2C%20delirium%2C%20and%20brain%20inflammation. - 13.
https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-long-term-effects/art-20490351 - 14.
Baig A, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: Tissue distribution, host-virus interaction, and proposed neurotropic mechanisms. ACS Chemical Neuroscience. 2020; 11 :995-998 - 15.
Olagunju AS, Oladapo IP, Kosemani SO, Olorunfemi FG, Adeyemo AS. Pathogenesis of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) respiratory infection. International Journal of Travel Medical Global Health. 2020; 8 (4):137-145. DOI: 10.34172/ijtmgh.2020.24 - 16.
Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARSCoV2 may be at least partially responsible for the respiratory failure of COVID-19 patients. Journal of Medical Virology. 2020; 92 :552-555 - 17.
Wrapp D, Wang N, Corbett K, et al. Cryo-EM structure of the 2019-nCoV spike in the prefusion conformation. Science. 2020; 367 :1260-1263 - 18.
Amruta N, Chastain WH, Paz M, Solch RJ, Murray-Brown IC, Befeler JB, et al. SARS-CoV-2 mediated neuroinflammation and the impact of COVID-19 in neurological disorders. Cytokine & Growth Factor Reviews. 2021; 58 :1-15. DOI: 10.1016/j.cytogfr.2021.02.002 - 19.
Ellul MA, Benjamin L, Singh B, Lant S, Michael BD, Easton A, et al. Neurological associations of COVID-19. Lancet Neurology. 2020; 19 (9):767-783 - 20.
Oxley T, Mocco J, Majidi S, et al. Large-vessel stroke as a presenting feature of Covid-19 in the young. The New England Journal of Medicine. 2020; 382 (20):e60 - 21.
Klok F, Kruip M, van der Meer N, Arbuos M, Gommers D, Kant K. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thrombosis Research. 2020; S0049-3848 (20):30120-30121 - 22.
Lodigiani C, Lapichino G, Carenzo L, Cecconi M, Ferrazzi P, Sebastian T. Venous and arterial thromboembolic complications in COVID 19 patients admitted to an academic hospital in Milan, Italy. Thrombosis Research. 2020; 191 :9-14 - 23.
Trejo-Gabriel-Galan JM. Stroke as a complication and prognostic factor of COVID-19. Neurología. 2020; 35 (5):318-322 - 24.
Yamana M, Kuwahara M, Fukumoto Y, Yoshikawa K, Takada K, Kusunoki S. Guillain-Barré syndrome and related diseases after influenza virus infection. Neurology: Neuroimmunology, Neuroinflammation. 2019; 6 :1-7. DOI: 10.1212/NXI.0000000000000575 - 25.
Bridwell R, Long B, Gottlieb M. Neurologic complications of COVID-19. The American Journal of Emergency Medicine. 2020; 38 (1549):e3-e7. DOI: 10.1016/j.ajem.2020.05.024 - 26.
Asiri S, Altwaijri WA, Ba-Armah D, Alrifai AARMT, Salam M, Almutairi AF. Prevalence and outcomes of Guillain-Barré syndrome among pediatrics in Saudi Arabia: A 10-year retrospective study. Neuropsychiatric Disease and Treatment. 2019; 15 :627-635. DOI: 10.2147/NDT.S187994 - 27.
Whittaker A, Anson M, Harky A. Neurological manifestations of COVID-19: A review. Acta Neurologica Scandinavica. 2020; 142 :14-22. DOI: 10.1111/ane.13266 - 28.
Jacobs B, Rothbarth P, van der Meche F, et al. The spectrum of antecedent infections in Guillain-Barre syndrome: A case-control study. Neurology. 1998; 51 :1110-1115 - 29.
Virani A, Rabold E, Hanson T, Haag A, Elrufay R, Cheema T. Guillain-Barré syndrome associated with SARS-CoV-2 infection. IDCases. 2020; 20 :e00771 - 30.
McGonagle D, Sharif K, O’Regan A, Bridgewood C. The role of cytokines including Interleukin-6 in COVID-19 induced pneumonia and macrophage activation syndrome-like disease. Autoimmunity Reviews. 2020; 19 (6):102537 - 31.
Wood H. Elevated risk of COVID-19 in people with dementia nature reviews. Neurology. 2021; 17 :194. DOI: 10.1038/s41582-021-00473-0 - 32.
Brown EE, Kumar S, Rajji TK, Pollock BG, Mulsant BH. Anticipating and mitigating the impact of the COVID-19 pandemic on Alzheimer's disease and related dementias. The American Journal of Geriatric Psychiatry. 2020; 28 (7):712-721 - 33.
Kubota T, Kuroda N. Exacerbation of neurological symptoms and COVID-19 severity in patients with preexisting neurological disorders and COVID-19: A systematic review. Clinical Neurology and Neurosurgery. 2021; 200 :106349 - 34.
Antonini A, Leta V, Teo J, Chaudhuri KR. Outcome of parkinson’s disease patients affected by COVID-19. Movement Disorders. 2020; 35 (6):905-908 - 35.
Hainque E, Grabli D. Rapid worsening in parkinson’s disease may hide COVID-19 infection. Parkinson Related Disordered. 2020; 75 :126-127 - 36.
Lo Monaco MR, Bentivoglio AR, Fusco D, Calabresi P, Piano C. Subacute onset dystonia in a woman affected by parkinson’s disease following SARS-COV-2 infection. Clinical Parkinsonism Related Disordered. 2021; 4 :100082-100082 - 37.
Cilia R, Bonvegna S, Straccia G, Andreasi NG, Elia AE, Romito LM, et al. Effects of COVID-19 on parkinson’s disease clinical features: A community-based case-control study. Movement Disorders. 2020; 35 (8):1287-1292 - 38.
Van der Heide A, Meinders MJ, Bloem BR, Helmich RC. The impact of the COVID-19 pandemic on psychological distress, physical activity, and symptom severity in parkinson’s disease. Journal of Parkinson's Disease. 2020; 10 (4):1355-1364 - 39.
Mortaz E, Malkmohammad M, Jamaati H, Naghan PA, Hashemian SM, Tabarsi P, et al. Silent hypoxia: Higher NO in red blood cells of COVID-19 patients. BMC Pulmonary Medicine. 2020; 20 (1):269 - 40.
Cafaro RP. Hypoxia: Its causes and symptoms. Journal of the American Dental Society of Anesthesiology. 1960; 7 (4):4-8 - 41.
Kennedy PGE. An overview of viral infections of the nervous system in the immunosuppressed. Journal of Neurology. 2021; 268 (8):3026-3030. DOI: 10.1007/s00415-020-10265-z - 42.
Koyuncu OO, Hogue IB, Enquist LW. Virus infections in the nervous system. Cell Host & Microbe. 2013; 13 (4):379-393. DOI: 10.1016/j.chom.2013.03.010 - 43.
Lan J, Ge J, Yu J, Shan S, Zhou H, Fan S, et al. Structure of the SARS-CoV-2 spike receptor-binding domain bound to the ACE2 receptor. Nature. 2020; 581 (7807):215-220. DOI: 10.1038/s41586-020-2180-5 - 44.
Fu J, Zhou B, Zhang L, Balaji KS, Wei C, Liu X, et al. Expressions and significances of the angiotensin-converting enzyme 2 gene, the receptor of SARS-CoV-2 for COVID-19. Molecular Biology Reports. 2020; 47 (6):4383-4392. DOI: 10.1007/s11033-020-05478-4 - 45.
Abdel Hafez SMN. Can Covid-19 attack our nervous system? Journal of Chemical Neuroanatomy. 2021; 117 :102006. DOI: 10.1016/j.jchemneu.2021.102006 - 46.
Beyerstedt S, Casaro EB, Rangel ÉB. COVID-19: Angiotensin-converting enzyme 2 (ACE2) expression and tissue susceptibility to SARS-CoV-2 infection. European Journal of Clinical Microbiology & Infectious Diseases. 2021; 40 :905-919. DOI: 10.1007/s10096-020-04138-6 - 47.
Zou X, Chen K, Zou J, Han P, Hao J, Han Z. Single-cell RNA-seq data analysis on the receptor ACE2 expression reveals the potential risk of different human organs vulnerable to 2019-nCoV infection. Frontiers of Medicine. 2020; 14 :185-192 - 48.
Qi F, Qian S, Zhang S, Zhang Z. Single cell RNA sequencing of 13 human tissues identify cell types and receptors of human coronaviruses. Biochemical and Biophysical Research Communications. 2020; 526 (1):135-140. DOI: 10.1016/j.bbrc.2020.03.044 - 49.
Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. International Journal of Oral Science. 2020; 12 (1):8. DOI: 10.1038/s41368-020-0074-x - 50.
Harmer D, Gilbert M, Borman R, Clark KL. Quantitative mRNA expression profiling of ACE 2, a novel homologue of angiotensin converting enzyme. FEBS Letters. 2002; 532 (1-2):107-110. DOI: 10.1016/s0014-5793(02)03640-2 - 51.
Devaux CA, Rolain J-M, Raoult D. ACE2 receptor polymorphism: Susceptibility to SARS-CoV-2, hypertension, multi-organ failure, and COVID-19 disease outcome. Journal of Microbiology, Immunology, and Infection. 2020; 53 :425-435. DOI: 10.1016/j.jmii.2020.04.015 - 52.
Kochi AN, Tagliari AP, Forleo GB, Fassini GM, Tondo C. Cardiac and arrhythmic complications in patients with COVID-19. Journal of Cardiovascular Electrophysiology. 2020; 31 (5):1003-1008. DOI: 10.1111/jce.14479 - 53.
Hamming I, Timens W, Bulthuis ML, Lely AT, Navis G, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. The Journal of Pathology. 2004; 203 :631-637. DOI: 10.1002/path.1570 - 54.
Song E, Zhang C, Israelow B, Lu-Culligan A, Prado AV, Skriabine S, et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. The Journal of experimental medicine, 2021; 218 (3):e20202135. DOI: 10.1084/jem.20202135 - 55.
Zhao Y, Zhao Z, Wang Y, Zhou Y, Ma Y, Zuo W. Single-cell RNA expression profiling of ACE2, the receptor of SARS-CoV-2. American Journal of Respiratory and Critical Care Medicine. 2020; 202 (5):756-759. DOI: 10.1164/rccm.202001-0179LE Erratum in: Am J Respir Crit Care Med. 2021 Mar 15;203(6):782 - 56.
Gemmati D, Bramanti B, Serino ML, Secchiero P, Zauli G, Tisato V. COVID-19 and individual genetic susceptibility/receptivity: Role of ACE1/ACE2 genes, immunity, inflammation and coagulation. Might the double X-chromosome in females Be protective against SARS-CoV-2 compared to the single X-chromosome in males? International Journal of Molecular Sciences. 2020; 21 (10):3474. DOI: 10.3390/ijms21103474 - 57.
Reza-Zaldívar EE, Hernández-Sapiéns MA, Minjarez B, Gómez-Pinedo U, Márquez-Aguirre AL, Mateos-Díaz JC, et al. Infection Mechanism of SARS-COV-2 and Its Implication on the Nervous System. Frontiers in immunology, 2021; 11 :621735. DOI: 10.3389/fimmu.2020.621735 - 58.
Bolay H, Gül A, Baykan B. COVID-19 is a real headache! Headache. 2020; 60 (7):1415-1421. DOI: 10.1111/head.13856 - 59.
Mao L, Jin H, Wang M, Hu Y, Chen S, He Q , et al. Neurologic manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurology. 2020; 77 (6):683-690. DOI: 10.1001/jamaneurol.2020.1127 - 60.
Ye M, Ren Y, Lv T. Encephalitis as a clinical manifestation of COVID-19. Brain, Behavior, and Immunity. 2020; 88 :945-946. DOI: 10.1016/j.bbi.2020.04.017 - 61.
Douaud G, Lee S, Alfaro-Almagro F, Arthofer C, Wang C, McCarthy P, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature, 2022; 604 (7907):697-707. DOI: 10.1038/s41586-022-04569-5 - 62.
Matschke J, Lütgehetmann M, Hagel C, Sperhake JP, Schröder AS, Edler C, et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurology. 2020; 19 (11):919-929. DOI: 10.1016/S1474-4422(20)30308-2 - 63.
Chen X, Laurent S, Onur OA, Kleineberg NN, Fink GR, Schweitzer F, et al. A systematic review of neurological symptoms and complications of COVID-19. Journal of Neurology. 2021; 268 (2):392-402. DOI: 10.1007/s00415-020-10067-3 - 64.
Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, et al. Neurologic features in severe SARS-CoV-2 infection. The New England Journal of Medicine. 2020; 382 (23):2268-2270. DOI: 10.1056/NEJMc2008597 - 65.
Nannoni S, de Groot R, Bell S, Markus HS. Stroke in COVID-19: A systematic review and meta-analysis. International Journal of Stroke. 2021; 16 (2):137-149. DOI: 10.1177/1747493020972922 - 66.
Majidi S, Fifi JT, Ladner TR, Lara-Reyna J, Yaeger KA, Yim B, et al. Emergent large vessel occlusion stroke during new York City's COVID-19 outbreak: Clinical characteristics and Paraclinical findings. Stroke. 2020; 51 (9):2656-2663. DOI: 10.1161/STROKEAHA.120.030397 - 67.
Barati F, Pouresmaieli M, Ekrami E, Asghari S, Ziarani FR, Mamoudifard M. Potential drugs and remedies for the treatment of COVID-19: A critical review. Biological Proceedings. 2020; 22 :15 - 68.
Smit M, Marinosci A, Agoritsas T, Calmy A. Prophylaxis for COVID-19: a systematic review. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases, 2021; 27 (4):532-537. DOI: 10.1016/j.cmi.2021.01.013 - 69.
Lv X, Li Z, Guan J, Zhang J, Xu B, He W, et al. ATN-161 reduces virus proliferation in PHEV-infected mice by inhibiting the integrin alpha5beta1-FAK signaling pathway. Veterinary Microbiology. 2019; 233 :147-153 - 70.
Sanders JM, Monogue ML, Jodlowski TZ, Cutrell JB. Pharmacologic treatments for coronavirus disease 2019 (COVID-19): A review. JAMA. 2020; 323 (18):1824-1836 - 71.
Zubair AS, McAlpine LS, Gardin T, Farhadian S, Kuruvilla DE, Spudich S. Neuropathogenesis and neurologic manifestations of the coronaviruses in the age of coronavirus disease 2019: A review. JAMA Neurology. 2020; 77 (8):1018-1027 - 72.
Manji H, Carr AS, Brownlee WJ, Lunn MP. Neurology in the time of COVID-19. Journal of Neurology, Neurosurgery, and Psychiatry. 2020; 91 (6):568-570