
Abstract
Post-infective fatigue is a major long-lasting complication of COVID-19. Among long COVID-19 survivors, the persistent fatigues experienced have had a significant impact on their physical health and mental health. Post-infective fatigue has been described as a loss of energy and a feeling of heaviness. Likewise, more evidence has highlighted the mental health component of fatigue triggered by subjectively minor physical and cognitive activities. These bouts of fatigue are commonly associated with mental health issues such as anxiety, depression, and sleep disorders. Ultimately, these mental health problems affect the quality of life of survivors. Although necessary public health efforts were directed at controlling the spread of COVID-19 and treating physical symptoms, it is crucial to backtrack, to develop inclusive mental health services for individuals plagued by post-COVID-19 fatigue.
Keywords
- fatigue
- long COVID-19
- anxiety
- depression
- sleep disorders
1. Introduction
Since the COVID-19 pandemic hit, we have continued to experience an aftershock beyond acute symptoms of the virus. In December 2019, an acute respiratory disease from Wuhan, China spread rapidly across the globe [1]. It was soon identified as the novel coronavirus which was named severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) [1]. On March 11, 2020, the disease was declared a pandemic by the World Health Organization [2]. The mode of transmission of this virus is usually from human to human commonly through air droplets, and this feature was responsible for its rapid and progressive outbreak [3]. As of May 1, 2022, 513 million people have been infected by the virus with 6.23 million deaths globally [3].
As a respiratory disease, the COVID-19 virus primarily affects the respiratory system [4]. Although other organs are involved, lower respiratory tract infection symptoms such as fever, dry cough, and dyspnea were commonly reported [4]. Other symptoms such as headache, dizziness, generalized weakness, vomiting, and diarrhea were also observed [4]. Like the virus, it was noted that the respiratory symptoms of COVID-19 could progress rapidly [5]. As such, the symptoms could vary from minimal to significant hypoxia with acute respiratory distress syndrome (ARDS) [5]. In addition to the progressive nature of the virus, the short duration for the onset of symptoms was an added disadvantage to the nature of COVID-19. In earlier reports, the time of onset of symptoms to development of ARDS-related hypoxia may be as short as 9 days [6]. Typically, these symptoms can prove to be fatal. Although mechanisms have been placed to ensure acute response and control the spread of the virus, some survivors still experience distress long after management [7]. Therefore, the management of COVID-19 from the acute phase may be the beginning of a long path to full recovery. Months following hospitalization and acute care, some symptoms still persist in the post-COVID-19 phase [8].
Post-Covid-19, also known as, long COVID is used to describe the persistence of symptoms, weeks or months after an acute infection of Covid-19 irrespective of the viral status [8]. This state can be continuous, relapsing or remitting in nature. Post-COVID-19 can be divided into two stages depending on the duration of symptoms. The first is post-acute COVID-19 where symptoms are more than 3 weeks but less than 12 weeks and the other, chronic COVID-19 where symptoms continue beyond 12 weeks [8, 9]. The commonly reported symptoms include fatigue, dyspnea, joint pain, chest pain, cough, skin rashes, palpitations, headache, diarrhea, and paresthesia [8]. Of these symptoms, post-infective fatigue is the most persistent and debilitating [10].
Post-infective fatigue syndrome (PIFS) is a persistent, severe fatigue after an infection that cannot be explained by other medical or psychiatric conditions, which has been present for at least 6 months and significantly affects daily functioning [11]. After the onset of COVID-19, prevalence rates of fatigue persisting for months ranged from 9% to 58% [11]. It is observed that an increasing number of previously fit young people continue to have persistent fatigue months after mild cases of COVID-19 [9, 12]. Although it is currently established in some post-COVID-19 individuals, PIFS is not unique to coronavirus [12]. According to Rudroff et al. [7], it is noticed that patients treated for viral infections may sustain functional limitations over long periods. Hence, in comparison to COVID-19, patients with severe acute respiratory syndrome (SARS) had similar symptoms and persistent fatigue that was observed months and years beyond the initial infection [7]. Following the SARS epidemic, the health outcomes of recovered patients were observed 3 months, 6 months, and 12 months after hospital discharge, the findings reported that 64% had fatigue at 3 months, 54% at 6 months, and 60% at 12 months [13]. It was also discovered that chronic fatigue was related to sleeping difficulties [13]. Other studies also reported that patients experienced myalgia, joint pain, and depressive symptoms in addition to their fatigue [14]. In addition to SARS, studies have reported a similar trend of persistent fatigue with influenza virus, Ebola virus, and West Nile virus months after they have recovered [11, 13]. There has also been a recognized link between viral symptoms and fatigue [15]. Anecdotal reports suggest that patients who do not recover fully from COVID-19 experience some lingering symptoms of fatigue. Likewise, studies suggest that COVID-19 has had an exacerbating effect among those with chronic fatigue syndrome [13].
Mental health symptoms such as depression and anxiety are identified to be related to post-COVID-19 [16, 17]. Studies support that there is an established link between fatigue and mental health problems [18]. Hence, among long-COVID patients or post-COVID-19 individuals, these symptoms were found present. Mental health disorders such as depression, anxiety, post-traumatic stress disorder, and sleep disorders were found to occur with the chronic and debilitating nature of the fatigue [19]. According to the DSM-V, these disorders are characteristically mental health disorders. Overall, these mental disorders, in addition to the physical impact of fatigue, result in a decline in the quality of life of individuals [20]. In COVID-19, since the public health focus was on safety and survival, the mental health issue has been widely overlooked [21]. A proper and proactive approach to the prevention and management of the mental disorders associated with post-COVID fatigue is necessary to improve the individual’s quality of life long after the onset of the disease.
2. Pathophysiology of post-COVID-19 fatigue
Typically, across various infections, symptoms of fatigue persist long after the onset of the disease [18]. Although the characteristics of chronic fatigue commonly associated with post-infectious diseases such as post-COVID-19 remain controversial, the manifestations remain similar to other post-infectious diseases irrespective of the pathogen. According to Poenaru et al. [17], the proposed mechanism of chronic fatigue in post-infection is likely multifactorial.
2.1 Immune/inflammatory mechanisms
In post-infectious fatigue, the immune system appears to be impacted by the pathogen [13]. The process remains unclear and can involve multiple pathways. A proposed mechanism is that during acute infection by the COVID-19 virus, tissue damage is sustained which results in the activation of auto-reactive bystander cells and molecular mimicry [16]. For example, in patients with severe COVID-19, there has been a substantial production of anti-nuclear antibodies. Also, rheumatic factor was detected among such individuals suggesting that there is increased activation of auto-reactive B-cells [16]. However, in chronic fatigue syndromes, antibodies that work against muscarinic and adrenergic receptors have been the syndrome but no auto-antibody has been linked to chronic antibodies [16].
Another mechanism purports that the deregulation of cytokine networks may play a role in chronic fatigue [8, 22]. A study on encephalitis detected those increased levels of pro-inflammatory cytokines were observed from the acute phase and remained consistently elevated 30 days post-infection within the central nervous system [16, 17]. However, evidence found no significant association between cytokine levels and chronic fatigue. Better still, new evidence suggested that cytokine signaling was more significant [16].
2.2 Mitochondrial function
Within the muscle tissue, alterations in mitochondrial structure, metabolism, and energy production may be associated with chronic fatigue [8, 11, 17]. Mitochondrial degeneration, pleomorphic features, and structural abnormalities were found in muscles of individuals diagnosed with post-viral symptoms [16]. From the onset of symptoms, mitochondrial enzymes are involved in the inflammatory and anti-oxidant pathways due to their involvement in peripheral vasodilation and autonomic regulation of the cardiovascular system [16]. This mechanism has not been evidence enough to link post-infectious chronic fatigue with mitochondrial dysfunction [8]. Also, a clear logical way to explain the pathway of lasting mitochondrial abnormalities among post-infectious individuals is also lacking [8].
2.3 Central nervous system involvement
Mental health symptoms such as sleep disorders and post-anxiety stress disorders commonly with chronic fatigue may reflect impairment of the central nervous system [21]. Many viruses, including coronaviruses, have been shown to cause damage to the CNS tissue [11, 21]. For example, SARS-CoV1, as well as COVID-19, has been associated with edema, neuronal degeneration, demyelination, and necrosis resulting in an increased risk for cerebral ischemic events. In addition, a high proportion of rapid eye movements and alpha electroencephalographic sleep disorders were found among SARS survivors who had chronic fatigue [16]. This is a common mechanism behind sleep disorders in post-infectious fatigue. Although this mechanism has been defined, the causal relationship between the infection, altered CNS structure, and chronic fatigue still remain unclear (Figure 1) [16].
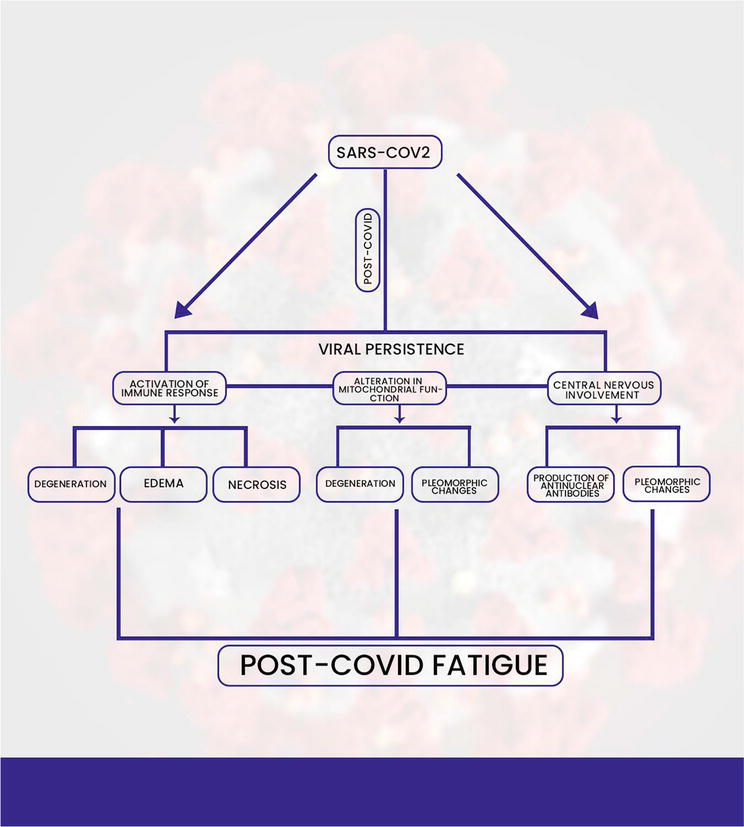
Figure 1.
The pathophysiology of post-COVID fatigue.
3. Effects of post-COVID 19 fatigue on mental health
There is an inconsequential effect of post-COVID-19 fatigue on the mental health of survivors [22]. Several factors such as reduced physical functioning, and social and economic issues that may trigger fatigue may subsequently cause mental health issues [22]. The history of pre-existing mental health problems may also aggravate the mental health issues activated by fatigue [21]. Mental health problems such as depression, anxiety, post-traumatic stress disorder, and sleep disorders are commonly related to symptoms of post-COVID-19 [23]. However, among people who have developed post-COVID-19 fatigue, the mental health problems are usually co-occurring and potentially codependent on post-COVID-19 fatigue [24]. A study on neuropsychological and neurophysiological correlates of fatigue in post-covid-19 patients supports that there was no significant correlation between apathy, depression, and fatigue. Although they were found to co-exist in post-COVID patients, they were not associated [25]. There is a paucity of literature on the direct impact of fatigue on mental health disorders. However, the effects on mental health were mainly a result of biological, psychosocial, and economic factors [25]. Reduced physical activity, which is an outcome of the chronic nature of post-COVID-19 fatigue influences the onset of or exacerbation of mental health problems [26]. Likewise, the mental component of fatigue, such as reduced motivation can influence developing mental health disorders [27].
4. Factors affecting the mental health impact of post-COVID fatigue
The mental health impact of post-COVID fatigue is typically a co-existing component of fatigue. However, contributing factors responsible for their onset or aggravation exists [7]. They include:
Biological factors: Serotonin and Dopamine play major roles in the mental/psychological aspects of fatigue. Among COVID-19 patients, COVID-19 may be transported via the olfactory bulb to the forebrain, which has a substantial amount of dopamine and serotonin [7]. This may alter the levels of dopamine and serotonin responsible for controlling moods and other affect [7]. These changes in the brain may be responsible for mental effects such as anxiety and depression among post-COVID-19 individuals [7].
Task dependent factors: this includes changes in fatigue that are dependent on the tasks performed. Fatigue is commonly triggered by specific cognitive or motor tasks performed [7]. The extent of the task persons, especially one that over-exerts the individual may trigger or aggravate the mental effects of the fatigue [7].
Environmental factors: This refers to how the environment affects the COVID-19 survivors from the acute phase and throughout the process of recovery [7]. For example, the financial implications of the pandemic or management, self-isolation, lockdown, and social isolation may contribute negatively to the individuals’ mental capacity. It has been reported by some earlier authors that the financial loss as a result of Covid-19, was associated with depression [7]. Therefore, the environmental and societal effects of the pandemic may be largely responsible for mental effects such as anxiety, depression, and post-traumatic stress disorders among post-COVID fatigued individuals [7].
Physical and Mental capacity: Initial physical capacity, that is, the prior state of well-being can be a contributing factor to the physical as well as the mental component of post-COVID fatigue [7]. In addition, an initial mental orientation about COVID-19, resulting in individuals’ experiencing anxiety and distress can lead to and aggravate the levels of fatigue [25]. In such cases, pre-existing medical conditions should also be considered as primary or supplementary causes of the mental effects of fatigue. Conditions such as cardiovascular diseases, diabetes, and chronic kidney disease may cause these populations to be affected by the persistent effects of fatigue in comparison to people with no co-morbid conditions [7].
5. Management of mental health issues related to post-COVID fatigue
Depression, anxiety and stress are common mental health issues that have been identified in COVID survivors [28]. While these mental health conditions may not be directly linked to post-COVID fatigue, they commonly co-exist in the study population. These mental health disorders have been reported to be effectively managed using a combination of psychological and pharmacological treatment methods [29].
In the management of people with depression, literature suggests psychotherapy by psychologists or psychiatrists, as the first line of management [29]. This includes behavioral activation (helping the individual to identify and adopt new routines that could motivate or make them happy); and guide them in the process of identifying the major problems responsible for the health status, as well as self-developing solutions to these problems [30, 31]. Self-help materials can also be provided for these individuals to guide and foster the development of healthy behaviors [29].
Furthermore, it is important that healthcare professionals monitor these individuals during the process of healing, to ensure that they achieve their set goals [32]. Considering the residual fatigue post-COVID, it is important that the gradual return to activities is stressed. This will help them slowly adjust to the energy demand of activities, while this keeping their goals in mind. A sudden return to strenuous activities (which may be top on their list) may be very difficult, if not impossible for some of them to achieve. If not properly managed, this may demoralize the patient further, or in extreme cases lead to a sequela of other events. In cases where the symptoms persist or reoccur after psychological intervention, antidepressants are prescribed [33]. Cleare et al. [34] suggests that people who suffer from severe depression should undergo both psychological and pharmacologic management from the onset to achieve the best treatment outcomes.
While healthcare professionals await comprehensive research and reports on how to manage patients with long-COVID symptoms, it is imperative that we continue to use the available methods such as cognitive behavioral therapy (CBT), and peer support to management patients who suffer from mental health conditions due to the COVID experience [34]. People who report symptoms of anxiety should be asked about the exact reason or source of worry. Management of their condition should begin by addressing these worries. It is also important to educate patients on making treatment goals. Using these goals as a guide in helping patients during psychotherapy sessions, to ensure return to activity. Patients should be asked to make a list of activities they would like to return to. These activities should then be ranked based on the level of anxiety they cause the client. The healthcare professional should then advice the client to gradually commence their ‘return to activity’ with activities that worry them the least.
In addition, pharmacological means have proven to be effective in the management of anxiety in this population. Class of medications such as selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, tricyclic antidepressants, benzodiazepenes, and gabapentinoids, among others have been successfully used in the management of anxiety [35]. Beyond the psychopharmacological treatment protocols, other conservative management techniques such as acupuncture, meditation, yoga, and exercise have been equally reported to be effective in managing anxiety in this population [35]. Exercises will steadily help to improve endurance, boost mood and improve immunity. Hence, I recommend exercises as an effective method of treating mental health issues in people with post-COVID fatigue.
Overall, due to the dearth of information on evidence-based techniques in managing mental health conditions in people suffering from long-COVID symptoms, mental health and rehabilitation experts have resorted to using the generally accepted methods to manage these conditions. So far, these are the best available approaches to help improve the quality of life of these individuals. However, it is necessary to view the patient holistically and take other symptoms (such as the co-existing fatigue) that the patients report into cognizance. This way, health care outcomes will be optimized. It is recommended that more mental health experts should carry out research to explore the effectiveness of various protocols in the management of mental health issues that are associated with post-COVID fatigue.
6. Consequences of neglecting the mental health impact of post-COVID fatigue
There is an overall decline in the quality of life of individuals as a result of a neglect of the mental health component of post-COVID 19 fatigue [36]. Commonly, the public health strategies focused on controlling the spread of and reducing the acute symptoms accompanying the virus [37]. These strategies have ranged from proper pharmacological management to the dissemination of COVID-19 vaccines [38]. However, as studies begin to report the symptoms of post-COVID-19 fatigue, the mental health impact is repeatedly highlighted [39, 40]. More often, post-COVID-19 fatigue and mental health effects such as sleep disorders, anxiety and depression, and post-traumatic stress disorders are co-occurring and sometimes associated with physical components [39, 40]. Therefore, when mental health becomes repeatedly overlooked, the overall quality of life of the individuals declines [36, 41]. For example, the mental health disorder may aggravate the physical component of fatigue, resulting in muscle weakness and reduction in cognition. This neglect can also have a disproportionate impact on other mental health consequences such as suicide [42]. In the United States of America, during the 2 months of lockdown, more suicides caused by mental health disorders were recorded than COVID-19 deaths. Likewise, poor coping mechanisms such as drug and alcohol abuse can be taken up to alleviate the mental health effects [43]. With these debilitating consequences, it is important that strategies are put in place to alleviate them.
7. Beyond the surge: strategies to address the mental health impact of post-COVID fatigue
Chronic fatigue experienced by some individuals who recovered from the COVID-19 infection may be a menace to its victims. It exposes people to new vulnerabilities that significantly impact their mental health status. Considering the widespread of the corona virus in the last two (2) years, it is imperative that its mental health effects are checked promptly to prevent an overwhelming surge in the prevalence of global mental health dysfunction.
Despite a surge in the mental health issues following the first few months of the pandemic, the World Health Organization (2020) reported a marked reduction in the delivery of and accessibility to mental health services. Nonetheless, mental health experts came up with new ways of rendering efficient mental health services to individuals who need it. By mid-2020, many developed nations had established the use of digital health means to deliver mental health care [44, 45]. Chew et al. [35] reported the effective use of digital health methods such as cloud-based big data systems, artificial intelligence (AI)–based chatbots, online health communities (OHCs), and telehealth platforms in mental healthcare delivery.
In 2020, the National Institute for Health and Care Excellence (NICE) [46] proposed the empowerment of individuals to return to the community fully and take charge of their own management with the help of a multidisciplinary rehabilitation team. Healthcare practitioners have identified the need for psychologists and physicians to collaborate to ensure the successful management mental health issues due to long-COVID [47]. A psychologist, Hardin reported the lack of an absolute treatment (surgery, or medication) that would instantly relieve the mental health symptoms experienced by survivors of the COVID-19 diseases [47]. She however opined that early intervention and provision of realistic advice to help patients manage their feelings during this period, may significantly impact the efficacy of treatment. Aiyegbusi et al. [48] suggested routine mental health screening as a part of the follow-up treatment for people suffering from post-COVID fatigue and other long-COVID syndromes. This will help healthcare providers to promptly identify individuals who are at risk and commence management early [48].
8. Conclusion
Summarily, post-COVID fatigue is a potentially debilitating condition that may negatively impact the quality of life of individuals. Although available evidence suggests that mental health conditions such as depression and anxiety that exist in individuals with long-COVID is not directly linked to chronic fatigue experienced by some members of this group, they often co-exist. This implies that the status of one may impact the other on the long run, hence, the need for them to both be managed effectively. Healthcare practitioners have worked tirelessly in the last few years to come up with efficient and effective methods to deliver mental health care to individuals who require them. However, the body of knowledge will be greatly improved if more research is done to explore this aspect of health care.
References
- 1.
Yuki K, Fujiogi M, Koutsogiannaki S. COVID-19 pathophysiology: A review. Clinical Immunology (Orlando, Fla.). 2020; 215 :108427 - 2.
Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta bio-medica: Atenei Parmensis. 2020; 91 (1):157-160 - 3.
Our World in Data. 2022. Available from: https://ourworldindata.org/explorers/coronavirus-data-explorer . [Accessed: May 1, 2022] - 4.
Alizadehsani R, Alizadeh Sani Z, Behjati M, Roshanzamir Z, Hussain S, Abedini N, et al. Risk factors prediction, clinical outcomes, and mortality in COVID-19 patients. Journal of Medical Virology. 2021; 93 (4):2307-2320 - 5.
Maveddat A, Mallah H, Rao S, Ali K, Sherali S, Nugent K. Severe acute respiratory distress syndrome secondary to coronavirus 2 (SARS-CoV-2). The International Journal of Occupational and Environmental Medicine. 2020; 11 (4):157 - 6.
Lin SH, Zhao YS, Zhou DX, Zhou FC, Xu F. Coronavirus disease 2019 (COVID-19): Cytokine storms, hyper-inflammatory phenotypes, and acute respiratory distress syndrome. Genes & Diseases. 2020; 7 (4):520-527 - 7.
Rudroff T, Fietsam AC, Deters JR, Bryant AD, Kamholz J. Post-COVID-19 fatigue: Potential contributing factors. Brain Sciences. 2020; 10 (12):1012 - 8.
Raveendran AV, Jayadevan R, Sashidharan S. Long COVID: an overview. Diabetes & Metabolic Syndrome: Clinical Research & Reviews. 2021; 15 (3):869-875 - 9.
Fernández-de-Las-Peñas C, Palacios-Ceña D, Gómez-Mayordomo V, Cuadrado ML, Florencio LL. Defining post-COVID symptoms (post-acute COVID, long COVID, persistent post-COVID): An integrative classification. International Journal of Environmental Research and Public Health. 2021; 18 (5):2621 - 10.
Smith A. Post-viral fatigue: Implications for long COVID. Asian Journal of Research in Infectious Diseases. 2021; 6 (1):17-23 - 11.
Vink-Niese A. Could cognitive behavioral therapy be an effective treatment for long COVID and post COVID-19 fatigue syndrome? Lessons from the Qure Study for Q-Fever Fatigue Syndrome. Healthcare (Basel Switzerland). 2020; 8 (4):552 - 12.
Verveen A, Müller F, Lloyd A, Moss-Morris R, Omland T, Penninx B, et al. A research agenda for post-COVID-19 fatigue. Journal of Psychosomatic Research. 2022; 154 :110726 - 13.
El Sayed S, Shokry D, Gomaa SM. Post-COVID-19 fatigue and anhedonia: A cross-sectional study and their correlation to post-recovery period. Neuropsychopharmacology Reports. 2021; 41 (1):50-55 - 14.
Islam MF, Cotler J, Jason LA. Post-viral fatigue and COVID-19: Lessons from past epidemics. Fatigue: Biomedicine, Health & Behavior. 2020; 8 (2):61-69 - 15.
Kamal M, Abo Omirah M, Hussein A, Saeed H. Assessment and characterization of post-COVID-19 manifestations. International Journal of Clinical Practice. 2021; 75 (3):e13746 - 16.
Townsend L, Dyer AH, Jones K, Dunne J, Mooney A, Gaffney F, et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. Plos One. 2020; 15 (11):e0240784 - 17.
Poenaru S, Abdallah SJ, Corrales-Medina V, Cowan J. COVID-19 and post-infectious myalgic encephalomyelitis/chronic fatigue syndrome: A narrative review. Therapeutic Advances in Infectious Disease. 2021; 8 - 18.
Zawadka-Kunikowska M, Zalewski P, Newton JL. The similarities between Long-haul COVID-19 and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Medical Research Journal. 2021; 6 (1):77-78 - 19.
Rupp I, Boshuizen HC, Jacobi CE, Dinant HJ, van den Bos GA. Impact of fatigue on health-related quality of life in rheumatoid arthritis. Arthritis Care & Research. 2004; 51 (4):578-585 - 20.
Simani L, Ramezani M, Darazam I. A, Sagharichi M, Aalipour M. A, Ghorbani F, Pakdaman H. Prevalence and correlates of chronic fatigue syndrome and post-traumatic stress disorder after the outbreak of the COVID-19. Journal of Neurovirology, 2021; 27 (1):154-159 - 21.
Shanbehzadeh S, Tavahomi M, Zanjari N, Ebrahimi-Takamjani I, Amiri-Arimi S. Physical and mental health complications post-COVID-19: Scoping review. Journal of Psychosomatic Research. 2021; 147 :110525 - 22.
Zürcher SJ, Banzer C, Adamus C, Lehmann AI, Richter D, Kerksieck P. Post-viral mental health sequelae in infected persons associated with COVID-19 and previous epidemics and pandemics: Systematic review and meta-analysis of prevalence estimates. Journal of Infection and Public Health. 2022; S1876-0341 (22):00090-00099 - 23.
Low RN, Low RJ, Akrami A. A cytokine-based model for the pathophysiology of long COVID symptoms. OSF Preprints. 2020. DOI: 10.31219/osf.io/7gcnv - 24.
Vollbracht C, Kraft K. Feasibility of vitamin C in the treatment of post viral fatigue with focus on long COVID, based on a systematic review of IV Vitamin C on fatigue. Nutrients. 2021; 13 (4):1154 - 25.
Mardani M. Post COVID syndrome. Archives of Clinical Infectious Diseases. 2020; 15 (2):e108819 - 26.
Rudroff T, Workman CD, Bryant AD. Potential factors that contribute to post-COVID-19 fatigue in women. Brain Sciences. 2022; 12 (5):556 - 27.
Tabacof L, Tosto-Mancuso J, Wood J, Cortes M, Kontorovich A, McCarthy D, et al. Post-acute COVID-19 syndrome negatively impacts physical function, cognitive function, health-related quality of life, and participation. American Journal of Physical Medicine & Rehabilitation. 2022; 101 (1):48 - 28.
Kathirvel N. Post COVID-19 pandemic mental health challenges. Asian Journal of Psychiatry. 2020; 53 :102430. DOI: 10.1016/j.ajp.2020.102430 - 29.
Abas MA. Combining active ingredients to treat depression in the wake of COVID-19. The Lancet Psychiatry. 2021; 93 (3):190-191 - 30.
Ekers D, Webster L, Van Straten A, Cuijpers P, Richards D, Gilbody S. Behavioural activation for depression; an update of meta-analysis of effectiveness and subgroup analysis. PLoS One. 2014; 9 :e100100 - 31.
Wampold BE. How important are the common factors in psychotherapy? An update. World Psychiatry. 2015; 14 :270-277 - 32.
Hides L, Carroll S, Lubman DL, Baker A. Brief motivational interviewing for depression and anxiety. In: Bennett-Levy J, Richards D, Farrand P, editors. Oxford Guide to Low Intensity CBT Interventions. USA: Oxford University Press; 2010. pp. 177-186 - 33.
Dunlop BW. Evidence-based applications of combination psychotherapy and pharmacotherapy for depression. Focus American Psychiatric Association Publishing. 2016; 14 :156-173 - 34.
Cleare A, Pariante CM, Young AH, et al. Evidence-based guidelines for treating depressive disorders with antidepressants: A revision of the 2008 British Association for Psychopharmacology guidelines. Journal of Psychopharmacology. 2015; 29 :459-525 - 35.
Uzunova G, Pallanti S, Hollander E. Presentation and management of anxiety in individuals with acute symptomatic or asymptomatic COVID-19 infection, and in the post-COVID-19 recovery phase. International Journal of Psychiatry in Clinical Practice. 2021; 25 (2):115-131 - 36.
Byrne A, Barber R, Lim CH. Impact of the COVID-19 pandemic–A mental health service perspective. Progress in Neurology and Psychiatry. 2021; 25 (2):27-33 - 37.
Ortelli P, Ferrazzoli D, Sebastianelli L, Engl M, Romanello R, Nardone R, et al. Neuropsychological and neurophysiological correlates of fatigue in post-acute patients with neurological manifestations of COVID-19: Insights into a challenging symptom. Journal of the Neurological Sciences. 2021; 420 :117271 - 38.
Bil JS, Buława B, Świerzawski J. Mental health and the city in the post-COVID-19 era. Sustainability. 2021; 13 (14):7533 - 39.
Adhikari SP, Meng S, Wu YJ, Mao YP, Ye RX, Wang QZ, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infectious Diseases of Poverty. 2020; 9 (1):1-12 - 40.
Chen X, Huang H, Ju J, Sun R, Zhang J. Impact of vaccination on the COVID-19 pandemic in US states. Scientific Reports. 2022; 12 (1):1-10 - 41.
Rao S, Benzouak T, Gunpat S, Burns RJ, Tahir TA, Jolles S, et al. Fatigue symptoms associated with COVID-19 in convalescent or recovered COVID-19 patients; a systematic review and meta-analysis. Annals of Behavioral Medicine. 2022; 56 (3):219-234 - 42.
Morgul E, Bener A, Atak M, Akyel S, Aktaş S, Jordan TR. COVID-19 pandemic and psychological fatigue in Turkey. International Journal of Social Psychiatry. 2021; 67 (2):128-135 - 43.
Vieira CM, Franco OH, Restrepo CG, Abel T. COVID-19: The forgotten priorities of the pandemic. Maturitas. 2020; 136 :38-41 - 44.
World Health Organization. The Impact of COVID-19 on Mental, Neurological and Substance Use Services: Results of a Rapid Assessment. Geneva: World Health Organization - 45.
Gratzer D, Torous J, Lam RW, Patten SB, Kutcher S, Chan S, et al. Our digital moment: Innovations and opportunities in digital mental health care. Canadian Journal of Psychiatry. Revue canadienne de psychiatrie. 2021; 66 (1):5-8. DOI: 10.1177/0706743720937833 - 46.
Kai CAM, Ryan O, Hsien-Hsien L, Rajendram M, Grisan KV, Verma SK, et al. Digital health solutions for mental health disorders during COVID-19. Frontiers in Psychiatry. 2020; 11 - 47.
Schreiber M. Treating patients with long COVID. American Psychological Association. 2021; 52 (5) - 48.
Aiyegbusi OL, Hughes SE, Turner G, et al. Symptoms, complications and management of long COVID: A review. Journal of the Royal Society of Medicine. 2021; 114 (9):428-442. DOI: 10.1177/01410768211032850