Open Access is an initiative that aims to make scientific research freely available to all. To date our community has made over 100 million downloads. It’s based on principles of collaboration, unobstructed discovery, and, most importantly, scientific progression. As PhD students, we found it difficult to access the research we needed, so we decided to create a new Open Access publisher that levels the playing field for scientists across the world. How? By making research easy to access, and puts the academic needs of the researchers before the business interests of publishers.
We are a community of more than 103,000 authors and editors from 3,291 institutions spanning 160 countries, including Nobel Prize winners and some of the world’s most-cited researchers. Publishing on IntechOpen allows authors to earn citations and find new collaborators, meaning more people see your work not only from your own field of study, but from other related fields too.
As a global threat, the COVID-19 pandemic is a challenge to psychological resilience. The aim was to determine the prevalence of various psychological disorders during the COVID-19 pandemic. This is a systematic review. Studies using different combinations of keywords COVID-19, SARS-COV, pandemic, psychological disorders, mental health and, psychological consequences were retrieved from different scientific databases Elsevier, Pubmed, Science Direct, Scopus, Web of Science. These studies were published from December 1, 2019, to May 30, 2020. Twenty-eight studies out of 410 retrieved articles were evaluated and analyzed for data extraction. The analysis of studies revealed that the different types of psychological disorders like stress, anxiety, depression, post-traumatic stress disorder, mental distress, schizophrenia, sleep disorders and sleep disturbances, vicarious traumatization, and internet addiction on moderate to severe in public and medical personnel were recorded during COVID-19 crisis. The frontline health care workers were more depressed, anxious, insomniac, and mentally disturbed. Women were more vulnerable to psychological disorders and sleep problems. Young people were more likely to experience generalized anxiety disorder and mental distress. COVID-19 has led to high prevalence and a wide range of psychological disorders in society. It is essential to provide psychological assistance and training strategies to deal with a variety of these psychological disorders.
Nursing Faculty, Behavioral Sciences Research Center, Life Style Institute, Baqiyattallah University of Medical Sciences, Tehran, Iran
Leila Karimi
Nursing Faculty, Behavioral Sciences Research Center, Life Style Institute, Baqiyattallah University of Medical Sciences, Tehran, Iran
*Address all correspondence to: khalili1120@gmail.com
1. Introduction
Coronavirus Disease 2019 [COVID-19] appeared in Wuhan, China in December 2019 and spread rapidly throughout the country and then the world, so today we are facing a pandemic [1]. From 15 April 2020 to 21 July 2022, a number of 571,833,637 Covid-19 patients were identified in the world, of which 6,396,439 deaths due to the virus occurred [2]. So far, this virus has caused 108,721,646 total infected cases and 1,499,042 total deaths in the USA. The most cases and mortality of 212,621,751 and 1,868,908 respectively, occurred after this pandemic in Europe. Also, in Asia, there have been 165,724,865 total cases and 1,444,347 total deaths due to this virus [2].
The ambiguous nature of the disease and its unfamiliarity, as well as the implementation of quarantine measures that were strictly applied in some countries, such as China, to keep a large number of people in isolation, increased the burden of the disease and affected many aspects of their lives. It has caused widespread psychological problems such as panic disorder, anxiety, and depression along with physical problems [3]. Sirati Nir mentions according to Wang & et al “Anxiety caused by the fear of being in the community causes people not to enter shopping centers, students do not enter educational centers, and workers and tourists do not enter work and leisure institutions, and these cases lead to feelings of reduced independence and stress and worries about income and security occupations and other issues have led to psychological problems, with governments in China, Singapore, and Australia expressing concern about the psychological side effects of Covid-19, and the long-term effects of this isolation and fear in society are considered serious threats to mental health” [4].
Psychiatric disorders are highly prevalent in medical illnesses. According to world health organization (WHO) figures, at least 52 million people worldwide suffer from severe mental illness and 150 million from severe mental disorders [5]. A mental disorder is a behavioral and psychological pattern that occurs in a person and is associated with a functional disorder caused by a biological disorder [social, psychological, genetic, physical, or chemical] [6]. In addition to the suffering and limitations that it creates for the individual, mental illness causes discrimination in social and professional activities due to the stigma of mental illness and thus imposes a heavy financial burden on society and the individual [7]. In a systematic review, it was reported that the quality of life of communities that suffer from Covid-19 is greatly reduced due to social distance [8].
Also, epidemic outbreaks can cause significant psychological stress that may lead to adverse effects on the quality of life and overall mental health of employees, which emphasizes the need to establish psychological support programs for medical workers during infectious disease outbreaks. It has been suggested that social support may be a powerful strategy to reduce the negative consequences of mental status faced by medical workers during infectious disease epidemics [9, 10]. In research on previous epidemics in recent years, a wide range of psychosocial effects on individuals at the individual, community, and Internationally reported at the time of the outbreak of infection [11]; so the flu outbreak, about 3–10% of the general public were concerned about being infected with the virus and the disease [12]. In the study of the Ebola outbreak, a wide range of psychosocial effects on individuals during the outbreak of infection were reported at the individual, national and international levels, and at the individual level, individuals seeking high fears of illness or death, feeling weak. They had experienced disability and social stigma [11]. Closing schools and businesses increased the negative emotions that people experienced. For example, during the outbreak of SARS, significant psychological effects were reported, especially in younger people than in older people [13, 14].
Because the coronavirus COVID-19 is a public health emergency of international concern, it poses a challenge to psychological resilience. According to the evidence ordinary people, patients, staff, and family members of patients and health workers are exposed to the psychological damage caused by the epidemic of the virus. Understanding the mental state of people exposed to psychological disorders can help professionals to provide targeted psychological interventions to improve the patient’s mental health. Also, it is necessary to provide evidence-based strategies to policymakers in any community to reduce the adverse psychological effects and psychiatric symptoms during an epidemic, which can lead to restrictive measures to control and alleviate psychological problems following or during the COVID-19 epidemic [15]. Due to the onset of the Covid-19 epidemic in China, evidence-based assessments and mental health interventions for patients and health care staff are relatively rare [16]. Therefore, conducting a systematic study by reviewing and combining all related documents can create a more complete picture of the dimensions of this problem in society. Coronavirus infection has been performed worldwide and has looked for symptoms such as depression, anxiety, insomnia and anxiety and potential risk factors associated with it, and can therefore provide a clear basis for intervention and implementation of mental health intervention policies for confronting this challenge efficiently and effectively.
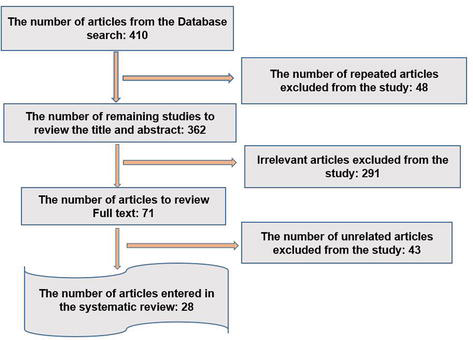
This study was conducted by systematic review. To access articles related to various types of psychological disorders in the face of the coronavirus covid-19 epidemic, articles published in databases such as Elsevier, Pubmed, Science Direct, Scopus, Web of Science, and Google Scholar search engines were used to search for articles using systematic search with the keywords Psychiatric consequences, Psychological disorder, Mental health problem, COVID-19, Outbreak in the period from 1 December to 30 May 2020. In addition, the reference list of the obtained articles was examined to identify the articles that were not obtained using the above methods. An initial search found 410 articles and then according to the title and abstract of articles and several levels and removal of unrelated and duplicate articles, finally 28 articles were included in the study for extraction and evaluation (Figure 1). Inclusion criteria included: main articles and studies on psychological disorders in the face of the Covid-19 coronavirus epidemic. Unknown reports from gray literature, book chapters, personal views, letters to the editor, historical articles, and non-scientific articles were excluded from this study. A screening tool for the quality of articles to select relevant articles PRISMA checklist was used. After collecting the relevant information was read by one of the authors and the most important points were summarized. The information was recorded in the standard format and then registered as a validity summary.
Figure 1.
The process of investigation, screening, and selection of articles.
Table 1 shows a summary of information from 28 evaluated articles on the prevalence of various psychological disorders in the face of the Corona Covid-19 pandemic. The items listed in Table 1 include the author and year of study, purpose, location, tools used, number of samples, population, study method, and related results. Based on Table 1, the types of psychological disorders following coronavirus can be categorized in different studies. All studies on the Covid-19 crisis in six countries, China, Iran, Iraq, India, Mexico, and the United Kingdom, were performed using standard tools using quantitative and qualitative methods. Of course, only a qualitative study was conducted in Iran [36]. Studies have been done only in the community [4, 18, 22, 25, 26, 27, 31, 33, 35, 36, 37, 39, 40]. A study has been done on the patients ‘families [20]. A study has been done exclusively in the patients’ community [15]. Studies have also been done on isolated people in the community [6, 17]. Also, studies have been done on the medical staff [19, 21, 23, 24, 28, 30, 32, 34, 38]. Studies have been conducted jointly between patients, the community, staff, and students [21, 22]. A study also shows a psychological comparison between the general public and nurses [30]. Schizophrenia, mental distress, insomnia and sleep disturbances, and Internet addiction were among the various studies. Anxiety levels of community members, patients, and treatment staff were reported to be moderate to severe in different studies of [6–65.6%] percent [4, 6, 15, 16, 17, 18, 21, 22, 23, 28, 29, 40]. Symptoms of depression were moderate to severe [8.4–50.4%] in isolated individuals, patients, medical staff, families of medical staff, and the affluent class of society [4, 15, 16, 17, 19, 20, 29].
Analysis of psychological state and clinical psychological intervention model of patients with COVID-19
Hamilton depression scale (HAMD) and Hamilton anxiety scale (HAMA)
Patients (113) and healthy people (30)/143
Experimental
The anxiety and depression score of patients admitted with Covid - 19 was higher than volunteers. After Psychological intervention dramatically anxiety and depression subsided.
Factors Associated With Mental Health Outcomes Among Health Care Workers Exposed to Coronavirus Disease 2019
Chinese versions of Patient Health Questionnaire, Generalized Anxiety Disorder scale, Insomnia Severity Index, and the 22-item Impact of Event Scale–Revised.
Nurse (764) and doctor (493)/1257
Cross -sectional
Severity of depressive symptoms; Anxiety and insomnia and psychological distress in 41.5% of medical staff on the front line Treatment at Wuhan hospitals Were higher than the others.
Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China
Event Scale-Revis Depression, Anxiety and Stress Scale (DASS-21)ed. (IES-R)
Adult citizen/1210
Cross -sectional
53.8% moderate to severe psychological disorders they had. 16.5% depression, 28.8% Anxiety, and 1.8% moderate to severe stress they had. Poor personal health status Wearing a mask and hand washing) with higher levels He was associated with psychological disorders.
Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China
General anxiety disorder (GHQ), Pittsburg Sleep Quality Index (PSQI), Center for Epidemiologic Scale- Depression (CES-D)
Health care worker and non Health care worker/603
Cross -sectional
34% of generalized anxiety, 18% of depression, and 18.1% reported sleep disorders. Persons with Younger Depression and more widespread anxiety And medical staff also had sleep disorders Showed more.
Mental health status among family members of health care workers in Ningbo, China during the Coronavirus Disease 2019 (COVID -19) outbreak
Chinese version of Patient Health Questionnaire-9 (PHQ-9) and the Chinese version of Generalized Anxiety Disorder-7(GAD-7)
Family of health care worker/822
Cross -sectional
33.7% reported generalized anxiety disorder and 3.29% reported depression. Family members who came in direct contact with suspected or positive Covid-19 cases were more prone to widespread anxiety.
Social Responses During the Early Stage of the COVID-19
The Hospital, Anxiety and Depression scale - Anxiety (HASD-A)
General population/1715
Cross-sectional
The majority (97%) were concerned about the prevalence of Covid-19, and 98% had a slight disturbance in their daily activities. Also, their anxiety score was on average abnormal.
Psychological Impact and Coping Strategies of Frontline Medical Staff in Hunan Between January and March 2020 During the Outbreak of Coronavirus Disease 2019 (COVID-19) in Hubei, China.
Researcher based Questionnaire (5 sections)
doctors, nurses, and other hospital staff/534
Cross-sectional observational study
The COVID-19 outbreak in Hubei resulted in increased stress for medical staff in adjacent Hunan province. Continued acknowledgment of the medical staff by hospital management and the government, provision of infection control guidelines, specialized equipment, and facilities for the management of COVID-19 infection should be recognized as factors that may encourage medical staff to work during future epidemics.
Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China.
General Health Questionnaire
Healthcare workers/4357
Cross-sectional study
Among the front-line staff at Wuhan Hospitals who were isolated and family members and co-workers had affected, there was a 39 percent psychological distress.
Prevalence and predictors of PTSS during COVID-19 Outbreak in China’s Hardest-hit Areas: Gender differences matter
PTSD Checklist for DSM-5, the Pittsburgh Sleep Quality Index (PSQI0), (PCL-5)
Residents of cities in crisis/285
Cross-sectional study
One month after the epidemic, the results showed that 7% of the study population had severe symptoms of post-epidemic stress. There were accidents (hyperexcitability, frequent reminders, and negative changes in mood and cognition). People with better sleep quality and early awakening had the fewest symptoms of post-traumatic stress.
prevalence of and risk factors for acute posttraumatic stress disorder (PTSD) in Chinese people shortly after the COVID-19 outbreak.
PTSD Checklist for DSM-5 (PCL-5), Sleep Quality Index (PSQI) (PCL-5)
Chinese people/2091
Cross-sectional study
One month after the epidemic, the results showed that 1.4% of the study population developed post-traumatic stress symptoms. Predictors of post-traumatic stress included the female population, people with a history of recent exposure in Wuhan, people at risk of infection, and poor sleep quality.
to validate this observation and find potential risk factors, if applicable
International Classification of Diseases 10th Edition (ICD-10)
Chines Adult population/13783
Cross-sectional study
After eliminating seasonal factors such as spring festivities, a positive relationship was found between the prevalence of schizophrenia and the Covid-19 epidemic for the first time. Also in the middle age group (39-50), a large increase in the incidence of schizophrenia was observed for the first time.
to evaluate sleep disturbances of fMW and made a comparison with non-fMW.
Pittsburgh Sleep Quality Index (PSQI), Athens Insomnia Scale (AIS) and Visual Analogue Scale (VAS)
medical workers from multiple hospitals in Hubei Province, China/1306
Cross-sectional study
Frontline staff had lower scores on sleep quality, insomnia, and depressive symptoms, and they were more anxious than other health care workers. Women showed lower sleep quality and more sleep disturbance than men compared to the subgroup.
Social capital and sleep quality in isolated individuals during the Covid-19 epidemic
Personal Social Capital Scale 16 (PSCI-16), Self-Rating Anxiety Scale (SRAS), the Stanford Acute Stress Reaction (SASR), Pittsburgh Sleep Quality Index (PSQI)
Isolated people For 14 days/170
Cross-sectional study
Low levels of social capital were associated with increased levels of anxiety and stress. But with increasing levels Social capital had a positive relationship with increasing the quality of sleep. Anxiety was associated with stress and decreased sleep quality, and the combination of anxiety and stress reduced the positive effects of social capital on sleep quality.
The effect of declaring the Covid-19 epidemic on psychological consequences
Online Ecological Recognition (OER)
Socially prosperous class/17865
Cross-sectional study
After the announcement of the Covid epidemic - 19 negative emotions (anxiety, depression, and violence) increased and vice versa positive emotions (life satisfaction and happiness) decreased. The subjects were most concerned about their own health and that of their families.
Adjacent psychiatric traumatization at the community level and medical and non-medical teams helping to control Covid-19
A mobile app-based
community members and nurses/730
cross-sectional study
Proximity psychological trauma was assessed with psychological and physiological scores among Frontline nurses were lower in treatment than nonlinear frontline nurses. The scores of proximity psychological trauma to the general public were higher than front-line nurses, but did not differ from non-front-line nurses.
Anxiety and depression in medical staff and the community
Hospital Anxiety and Depression Scale (HADS)
General population/2045
Descriptive- cross- sectional
65.6% and 423% of the samples had moderate to severe anxiety and depression, respectively. The prevalence of anxiety was higher in the age range of 30-39 years. Anxiety and depression in doctors, nurses, and people suspected of having Covid-19 were higher than in other occupations and the general public.
Factors related to the psychological state of individuals in Covid-19
Hospital Anxiety and Depression Scale (HADS)
Adult General population/788
Descriptive- cross –sectional
Mean anxiety and depression scores of the samples, respectively; were 7/08 ± 3.68 and 6.27 ± 71.3. Anxiety and depression scores were higher in widows, women, and those with cardiovascular disease.
Fear of death, anxiety, depression and decreased social activity and feelings of exclusion from society and reduced contact with family and community and the experience of the social stigma of having Covid-19 disease in the individual or family members were expressed.
Depression, Anxiety, and Stress in the Time of COVID-19 Pandemic in Kurdistan Region, Iraq. Kurdistan Journal of Applied Research
Depression, Anxiety and Stress Scale (DASS-21)
Adult General population/548
Descriptive- cross- sectional
45% had depression, 47% anxiety, and 18% stress. In regression analysis, the female gender was the most important factor for the high level of depression, anxiety, and stress. Depression, anxiety, and stress were higher in people with higher education.
Anxiety, depression, attitudes, and internet addiction during the initial phase of 2019 coronavirus disease (COVID-19) epidemic
Hospital Anxiety and Depression Scale (HADS), Internet Addiction Test (IAT)
Adult General population/561
Descriptive- cross –sectional
Fifty percent had anxiety, 27.6 percent had depression, and 62.7 percent had Internet addiction in the first few weeks of quarantine. Anxiety, depression in young people, and people addicted to the Internet with sleep problems were more.
Mental health during COVID-19 lockdown: A comparison of Austria and the UK. Available
Depression (PHQ-9), anxiety (GAD-7), stress (PSS-10), and sleep quality (ISI)
Adult General population/2015
Descriptive- cross –sectional
8.4% and 24.6% had severe depression in Astaria and England, 6% and 18.9% had severe anxiety in Austria and the UK, respectively, and 15.8% and 28.2% in the UK had sleep problems following COVID-19. The average perceived stress score in Staria and England was 16 ± 7.5 and 17.7 ± 7/9 respectively.
Table 1.
Summary of studies.
Generalized anxiety disorder also occurs in medical and non-medical staff and the families of medical staff [34%] were reported [19, 20]. Stress levels in isolated individuals, affluent class, and the general public were expressed from [8.1% to 73.4%] [6, 25]. A study was shown on adults in the community aged 39–50 years [27]. Psychological disturbance and distress were reported in quarantined and isolated individuals, the general adult population, and the medical staff on average to severe [39.1–71.5%] [16, 17, 18, 24, 33]. Internet addiction was also reported [62.7%] [39]. Sleep disorders were shown as low quality of sleep and insomnia in the community, medical and non-medical staff about [18.1–36.1%] [6, 19, 21, 25, 26, 27, 28, 39]. Vicarious traumatization was also, reported in a study in community, frontline, and non-front line nurses [30], so in community and non-frontier nurses who suffered from psychological damage in the form of symptoms of loss of appetite, fatigue, irritability, fear, inattention, numbness, despair, and insomnia were expressed. Behavioral disorders such as violence and aggression were reported in the affluent class of society [29, 32]. Psychosocial consequences following having Covid-19 disease in an individual or family member were reported in a study in Iran [36]. In some community studies, women were more vulnerable to psychological and sleep disorders [17, 23, 28, 31, 34, 35, 37]. Unemployed people [25%] also suffered from anxiety and psychological distress [18]. The level of psychological distress in Iranians with an average of [34.54] and a standard deviation was [14.92] which was higher than the average level of stress in Chinese with a value of 23.65 with a standard deviation of [5.45] [33]. Also, in front-line staff studies, about [41.5] were more likely to suffer from depression, anxiety, insomnia, and mental distress [16, 23, 28]. In some studies, younger people were more prone to generalized anxiety disorder and psychological distress [17, 19, 31, 39]. This study aimed to investigate the prevalence of various psychological disorders in the face of the coronavirus Covid-19 pandemic. Based on the results, the prevalence of various mental disorders was studied in 28 studies. In these studies, different groups including patients, patients’ families, healthy people in the community, and medical staff were examined. Most of the 28 studies on the prevalence of mental disorders and related factors were related to the general public [13 studies] and medical staff [9 studies].
The most common mental disorders in the studied studies were depression and anxiety disorders so the level of anxiety in the community, patients, and medical staff were reported in different studies from moderate to severe [6–65.6%] [4, 6, 15, 16, 17, 21, 22, 23, 28, 29, 40]. Generalized anxiety disorder was also reported in medical and non-medical staff and the families of medical staff [about 34%] [19, 20]. The use of measures such as accurate updating of health information, especially about the number of people who have improved, has been associated with low- stress levels in the Covid-19 epidemic in Chinese society. Additional information about medications or vaccines, transmission routes, and updates on the number of infected cases and locations [e.g., real-time, online tracking map] were also associated with lower levels of anxiety [20], which can be of interest to the health authorities of other communities in the Covid-19 epidemic. In this study, the prevalence of moderate to severe anxiety was in the community, patients, and medical staff and the anxiety of medical staff was higher than normal in the community. Psychological problems such as anxiety, fear, and stress are more common in patients with Covid-19 or people who suspect it and the families of these patients or those with whom they are in contact. Epidemiologists, doctors, and all health professionals can also be affected by these disorders [22]. Also, the results of the above studies showed that nurses are more vulnerable to serious psychological damage in their work environment than physicians and other treatment staff [28]. Consistent with the findings of the present study, the results of a study during the SARS epidemic in Taiwan showed that nurses suffered from severe psychological problems such as anxiety and depression and militancy, and mental distress [3, 41]. Also during the MERS-CoV epidemic in Saudi Arabia, nurses became frightened and nervous after experiencing stressful patient care experiences [42]. However, in this study, compared to previous studies, the percentage of mental disorders is higher.
The aim of this study was to investigate the prevalence of various psychological disorders in face of the coronavirus Covid-19 epidemic. Based on the results, the prevalence of various mental disorders was evaluated in 28 studies. In these studies, different groups including patients, patients’ families, healthy people in the community, and medical staff were examined. Most of the 28 studies on the prevalence of mental disorders and related factors were related to the general public (13 studies) and medical staff (9 studies). The most common mental disorders in the studied studies were Depression and Anxiety Disorder, so the level of anxiety in the community, patients, and staff were reported in various studies from moderate to severe (6–65.6%) [6, 21, 22, 23, 28, 29, 40, 15, 16, 17, 18, 19]. Disseminated anxiety disorder was also reported in medical and non-medical staff and about 34% of the staff of medical staff [19, 20]. Particularly in terms of the number of people who recovered, the low level of stress in the Covid-19 epidemic was associated with 19 Chinese communities. Additional information about drugs or vaccines, routes of transmission, and updates on the number of infected cases and location (e.g., real-time, map Online tracking) was also associated with lower levels of anxiety [20], which could be of concern to health officials in other communities in the Covid-19 epidemic.
In this study, the prevalence of moderate to severe anxiety was in the community, patients, and medical staff and the anxiety of medical staff were higher than normal in the community. Psychological problems such as anxiety, fear, and stress are often present in patients with Covid-19 or people who suspect it and the families of these patients or those with whom they are in contact. Also, epidemiologists, physicians, and all health professionals can be affected [22]. The results of the above studies also showed that nurses are more psychologically exposed to serious psychological damage in their work environment than physicians and other medical staff [28]. Results of the present study The results of a study during the SARS epidemic in Taiwan showed that nurses suffered from severe psychological problems such as anxiety, depression, militancy, and mental distress [3, 41]. Patients were taken care of, but in this study, compared to previous studies, the percentage of mental disorders is higher.
Another finding of the study was the higher prevalence of anxiety, depression, and stress in quarantined people, patients, treatment staff, and families of treatment staff as well as the affluent segment of society (8.1–73.4%) [4, 6, 17]. Similar to this finding, other studies have found long-term quarantine to cause psychological problems, including anxiety and depressive disorder [11]. People who are quarantined at home avoid stress and feel lonely due to lack of space for physical activity, stress due to limited social interactions, and anxiety due to fear of transmitting the infection to family members, so their mental health needs more attention [43]. Other studies have also found that social support and social activity in the community are effective in reducing the level of depression and anxiety and better mental health [6, 44]. Post-traumatic stress disorder was also reported at approximately (4.6–7%) among adults living in cities affected by the Covid-19 epidemic crisis. Other studies have noted this point that many quarantined people have experienced psychological distress, including post-traumatic stress disorder (PTSD) and depression, and the longer they are quarantined, the more likely they are to experience PTSD symptoms [6]. In most of the studies, a high percentage of the general public (97%) were concerned about the prevalence of Covid-19 and 98% had a slight disturbance in their daily work and life, as well as an anxiety score. On the contrary, the results of this study were conducted during a study of the H1N1 flu outbreak. The results showed that about 10–30% of the general public were concerned about being infected with the virus and the disease [12]. Decreased contact with family and community and experience of the social stigma of having Covid-19 disease in the individual or family members were also reported in a qualitative study in Iran [36].
In a study of the Ebola outbreak, a wide range of psychosocial effects was reported on individuals during an outbreak of infection, including fear of illness or death, feelings of weakness, disability, and social stigma [11]. In most of the studies, women were more vulnerable to psychological disorders and sleep disorders [18, 23, 28, 31, 34, 35, 37]. Although the prevalence of the disease in Iran was higher in men in than women [45], the results of the present study with most studies in Iran and The world, including the study of Ahmadvand, Khosravi, and Meyer, is consistent [46, 47, 48]. Evidence suggests that the higher prevalence of mental disorders in women than men may be more related to women ‘s limitations in social participation, biological factors, and environmental stress [49]. A history of positive contact with people with symptoms and people with higher education were more aware of the risk of SARS and had moderate anxiety levels and took more precautions [14]. They performed against the infection, which is somewhat different from the results of this epidemic. In some studies, young people were more prone to generalized anxiety disorder and mental distress [18, 19, 31, 39]. That people experience more, also during the outbreak of SARS, significant psychological effects have been reported, especially in young people compared to older people [13, 50], which is similar to the results of our study. The findings of the study emphasize the need to pay attention to the health of people who have not been affected by the virus, especially those who quit when the disease broke out or people who are active in sports, who have been forced to stop physical activity due to the outbreak of the disease. Also, people who are healthy themselves but have been in contact with infected people through family or work relationships because they had lower health, more anxiety, and less life satisfaction [18], as well as support for patients, family members, and providers. Health services during the epidemic were among the items mentioned in the studies. Things like paying more attention to vulnerable groups such as youth, the elderly, women, and migrant workers, accessing and strengthening medical resources, and the public health service system, especially after the initial midwifery examination and management of the Covid-19 epidemic. Nationwide strategy and coordination for psychological first aid during major disasters, which potentially.
Presented through medicine Telemedicine is one of the interventions that should be established, and finally, a comprehensive program to reduce stress should be designed through prevention and intervention including epidemiological monitoring, screening, referral, and targeted intervention to prevent further mental health problems [23]. Research timing can explain the difference in results. For the reasons mentioned above, what seems to increase the prevalence of mental disorders in the treatment of coronary heart disease is the application of traffic regulations, followed by the closure of recreational and sports facilities, unemployment, and the resulting economic pressures. He noted the low income of some citizens. According to the results of studies and the impact of COVID-19 disease in different segments of society, including patients, the general public, medical staff, and their families, it is necessary to do timely and effective psychological interventions. In addition to medical care for patients, especially pneumonia patients who need serious quarantine, the detection of psychological problems in the disease process online, is emphasized [21]. During the Corona epidemic in some countries, including China, psychological counseling services, including the telephone and, the Internet for counseling or intervention programs, became widespread, and the China Provincial Council announced that it was launching online institutions in response to the outbreak [49].
One of the limitations of the present study is that all research has been done in a short period of time, and due to the fact that new studies on the psychological consequences of this disease are updated every day, we were able to publish the studies until the end. May 2019 and evaluate in this study. However, due to a large number of participants and the study population, which has been done among all classes, including patients, medical and non-medical staff, patients’ families, quarantined people, and adults in general, this limitation is largely overshadowed.
According to the findings of the present study, Covid-19 causes a high prevalence and a wide range of psychological disorders such as (stress, anxiety, depression, post-traumatic stress disorder, schizophrenia, psychological distress, insomnia and sleep disturbance, and Internet addiction) in different individuals and groups. And especially the treatment and care staff. Because treatment and care staff are at the forefront of this incident, hospitals should strive to provide psychological support to nurses and provide timely psychological assistance and training to deal with the problem by empowering nurses to manage emotions and effective coping strategies. Other people in the community and patients also need training and support to deal with the psychological effects of the disease.
The Clinical Research Development Unit of Baqiyatallah Hospital, Behavioral Sciences Research Center, and the Vice Chancellor for Research, School of Nursing, Baqiyatallah University of Medical Sciences are hereby thanked and appreciated.
1.Xiao C. A novel approach of consultation on 2019 novel coronavirus (COVID-19)-related psychological and mental problems: Structured letter therapy. Psychiatry Investigation. 2020;17(2):1756. DOI: 10.30773/pi.2020.0047
2.World meters. 2020
3.Xiao H, Zhang Y, Kong D, Li S, Yang N. Social capital and sleep quality in individuals who selfisolated for 14 days during the coronavirus disease 2019 (COVID-19) outbreak in January 2020 in China. Medical Science Monitor. 2020:26. DOI: 10.12659/MSM.923921
4.Sirati Nir M, Karimi L, Khalili R. Research paper the perceived stress level of health care and non-health care in exposed to covid-19 pandemic. Iranian Journal of Psychiatry and Clinical Psychology. 2020;26(3 Spec):294-305. DOI: 10.32598/ijpcp.26.3405.1
5.WHO organization of mental health services in developing. Countries sixteen report of WHO. Available from: http://www.healthnettpo.org/mentalhealth
6.Cumbie SA, Conley VM, Burman ME. Advanced practice nursing model for comprehensive care with chronic illness: Model for promoting process engagement. Advances in Nursing Science. 2004;27(1):70-80. DOI: 10.1097/00012272-200401000-00008
7.Kaplan H SBAocpTbPN. Abstract of Clinical Psychiatry. 1st ed. Tehran: Hayyan; 1996
8.Melo-Oliveira ME, Sá-Caputo D, Bachur JA, Paineiras-Domingos LL, Sonza A, Lacerda AC, et al. Reported quality of life in countries with cases of COVID19: A systematic review. Expert Review of Respiratory Medicine. 2021;15(2):213-220. DOI: 10.1080/17476348.2021.1826315
9.Chen R, Chou KR, Huang YJ, Wang TS, Liu SY, Ho LY. Effects of a SARS prevention programme in Taiwan on nursing staff's anxiety, depression and sleep quality: A longitudinal survey. International Journal of Nursing Studies. 2006;43(2):215-225. DOI: 10.1016/j.ijnurstu.2005.03.006
10.Marjanovic Z, Greenglass ER, Coffey S. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: An online questionnaire survey. International Journal of Nursing Studies. 2007;44(6):991-998. DOI: 10.1016/j.ijnurstu.2006.02.012
11.Hall RC, Hall RC, Chapman MJ. The 1995 Kikwit Ebola outbreak: lessons hospitals and physicians can apply to future viral epidemics. General Hospital Psychiatry. 2008;30(5):446-452. DOI: 10.1016/j.genhosppsych.2008.05.003
12.Rubin GJ, Potts H, Michie S. The impact of communications about swine flu (influenza A H1N1v) on public responses to the outbreak: Results from 36 national telephone surveys in the UK. Health Technology Assessment. 2010;14(34):183-266. DOI: 10.3310/hta14340-03
13.Sim K, Chan YH, Chong PN, Chua HC, Soon SW. Psychosocial and coping responses within the community health care setting towards a national outbreak of an infectious disease. Journal of Psychosomatic Research. 2010;68(2):195-202. DOI: 10.1016/j.jpsychores.2009.04.004
14.Leung G, Lam T, Ho L, Ho S, Chan B, Wong I, et al. The impact of community psychological responses on outbreak control for severe acute respiratory syndrome in Hong Kong. Journal of Epidemiology & Community Health. 2003;57(11):857-863. DOI: 10.1136/jech.57.11.857
15.Yang L, Wu D, Hou Y, Wang X, Dai N, Wang G, et al. Analysis of psychological state and clinical psychological intervention model of patients with COVID-19. MedRxiv. 2020 Jan 1. DOI: 10.1101/2020.03.22.20040899
16.Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open. 2020;3(3):e203976. DOI: 10.1001/jamanetworkopen.2020.3976
17.Qiu J, Shen B, Zhao M. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. General Psychiatry. 2020;33(2):e100213. DOI: 10.1136/gpsych-2020-100213
18.Zhang SX, Wang Y, Rauch A, Wei F. Health, distress and life satisfaction of people in China one month into the COVID-19 outbreak. Distress and Life Satisfaction of People in China One Month into the COVID-19 Outbreak (3/12/2020). 2020 Mar 12. DOI: 10.2139/ssrn.3555216
19.Huang Y, Zhao N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 epidemic in China: A web-based crosssectional survey. medRxiv. 2020. DOI: 10.21203/rs.3.rs-17172/v1
20.Ying Y, Ruan L, Kong F, Zhu B, Ji Y, Lou Z. Mental health status among family members of health care workers in Ningbo, China, during the coronavirus disease 2019 (COVID-19) outbreak: a cross-sectional study. BMC psychiatry. Dec 2020;20(1):1-0. DOI: 10.1101/2020.03.13.20033290
21.Liu S, Yang L, Zhang XY, Liu Z. Servicios de salud mental en línea en China durante el brote de COVID-19. The Lancet Psychiatry. 2020;7(4):E17-8. DOI: 10.1016/ S2215-0366(20)30077-8
22.Kwok KO, Li KK, Chan HH, Yi YY, Tang A, Wei WI, et al. Community responses during early phase of COVID-19 epidemic, Hong Kong. Emerging infectious diseases. Jul 2020;26(7):1575. DOI: 10.1101/2020.02.26.20028217
23.Jiang Y. Psychological Impact and Coping Strategies of Frontline Medical Staff in Hunan Between January and March 2020 During the Outbreak of Coronavirus Disease 2019 (COVID 19) in Hubei, China. Medical Science Monitor. 2020;26:e924171. DOI: 10.12659/ MSM.924171
24.Dai Y, Hu G, Xiong H, Qiu H, Yuan X. Psychological impact of the coronavirus disease 2019 (COVID-19) outbreak on healthcare workers in China. medRxiv. 2020. DOI: 10.1101/2020.03.03.20030874
25.Liu N, Zhang F, Wei C, Jia Y, Shang Z, Sun L, et al. Prevalence and predictors of PTSS during COVID-19 Outbreak in China Hardest-hit Areas: Gender differences matter. Psychiatry Research. May 2020;287:112921. DOI: 10.1016/j.psychres.2020.112921
26.Sun L, Sun Z, Wu L, Zhu Z, Zhang F, Shang Z, et al. Prevalence and risk factors of acute posttraumatic stress symptoms during the COVID-19 outbreak in Wuhan, China. MedRxiv. 23 Apr 2020;10(2020.03):06-20032425. DOI: 10.1101/2020.03.06.20032425
27.Hu W, Su L, Qiao J, Zhu J, Zhou Y. COVID-19 outbreak increased risk of schizophrenia in aged adults. 2020;1:2-4
28.Qi J, Xu J, Li BZ, Huang JS, Yang Y, Zhang ZT, et al. The evaluation of sleep disturbances for Chinese frontline medical workers under the outbreak of COVID-19. Sleep medicine. 1 Aug 2020;72:1-4. DOI: 10.1101/2020.03.06.20031278
29.Li S, Wang Y, Xue J, Zhao N, Zhu T. The impact of COVID-19 epidemic declaration psychological consequences. A Study on Active on Weibo Usres. 2020:17(6);2032. DOI: 10.3390/ ijerph17062032
30.Li Z, Ge J, Yang M, Feng J, Qiao M, Jiang R, et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain, behavior, and immunity. 1 Aug 2020;88:916-919. DOI: 10.1101/2020.02.29.20029322
31.Moghanibashi-Mansourieh A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian Journal of Psychiatry . Jun 2020;51:102076. DOI: 10.1016/j. ajp.2020.102076
32.Taghizadeh F, Hassannia L, Moosazadeh M, Zarghami M, Taghizadeh H, Dooki AF, et al. Anxiety and depression in health workers and general population during COVID19 Epidemic in IRAN: A web-based cross-sectional study. medRxiv. 2020 Jan 1. DOI: 10.1101/2020.05.05.20089292
33.Jahanshahi AA, Dinani MM, Madavani AN, Li J, Zhang SX. The distress of Iranian adults during the Covid-19 pandemic–More distressed than the Chinese and with different predictors. Brain, behavior, and immunity. Jul 2020;87:124. DOI: 10.1016/j. bbi.2020.04.081
34.Kaveh M, Davari-tanha F, Varaei S, Shirali E, Shokouhi N, Nazemi P, et al. Anxiety levels among Iranian health care workers during the COVID-19 surge: A cross-sectional study. MedRxiv. 2020 Jan 1. DOI: 10.1101/2020.05.02.20089045
35.Ansari Ramandi MM, Yarmohammadi H, Beikmohammadi S, Hosseiny Fahimi BH, Amirabadizadeh A. Factors affecting the psychological status of an Iranian population during Coronavirus pandemic. Caspian Journal of Internal Medicine. 2020;11(1):2-0
36.Eisazadeh F, Aliakbari Dehkordi M, Aghajanbigloo S. Psychological consequences of patients with coronavirus (COVID-19): A qualitative study. Biquarterly Iranian Journal of Health Psychology. 2020;2(2):9-20
37.Othman N. Depression, anxiety, and stress in the time of COVID-19 pandemic in Kurdistan region, Iraq. Kurdistan Journal of Applied Research. 5 May 2020:37-44. DOI: 10.24017/covid.5
38.Vidyadhara S, Chakravarthy A, Kumar AP, Harsha CS, Rahul R. Mental health status among the South Indian Pharmacy students during Covid-19 pandemic’s quarantine period: a cross-sectional study. MedRxiv. 2020 Jan 1. DOI: 10.1101/2020.05.08.20093708
39.Priego-Parra BA, Triana-Romero A, Pinto-Gálvez SM, Ramos CD, Salas-Nolasco O, Reyes MM, et al. Anxiety, depression, attitudes, and internet addiction during the initial phase of the 2019 coronavirus disease (COVID-19) epidemic: A cross-sectional study in México. MedRxiv. 2020 Jan 1. DOI: 10.1101/2020.05.10.20095844
40.Pieh C, Budimir S, Probst T. Mental health during COVID-19 lockdown: A comparison of Austria and the UK. SSRN Electronic Journal. May 2020;10. DOI: 10.2139/ssrn.3592372
41.Chen WK, Cheng YC, Chung YT, Lin CC. The impact of the SARS outbreak on an urban emergency department in Taiwan. Medical care. 1 Feb 2005:168-172. DOI: 10.1097/00005650- 200502000-00010
42.Khalid I, Khalid TJ, Qabajah MR, Barnard AG, Qushmaq IA. Healthcare workers emotions, perceived stressors and coping strategies during a MERS-CoV outbreak. Clinical Medicine & Research. 2016;14(1):7-14. DOI: 10.3121/cmr.2016.1303
43.Valencia-Garcia D, Simoni JM, Alegría M, Takeuchi DT. Social capital, acculturation, mental health, and perceived access to services among Mexican American women. Journal of Latina/o Psychology. 2012;1(S):78-89. DOI: 10.1037/2168-1678.1.S.78
44.Li C, Jiang S, Fang X. Effects of multidimensional social capital on mental health of children in poverty: An empirical study in Mainland China. Journal of Health Psychology. 2020;25(6):853-867. DOI: 10.1177/1359105317737608
45.Farnoosh G, Ghanei M, Khorramdelazad H, Alishiri G, Farahani AJ, Shahriary A, et al. Are Iranian sulfur mustard gas-exposed survivors more vulnerable to SARS-CoV-2? Some similarity in their pathogenesis. Disaster medicine and public health preparedness. Dec 2020;14(6):826-832. DOI: 10.1017/dmp.2020.156
46.Meyer C, Rumpf H, Hapke U, Dilling H, John U. Lifetime prevalence of mental disorders in general adult population. Results of TACOS study. Der Nervenarzt. 2000;71(7):535-542. DOI: 10.1007/s001150050623
47.Ahmadvand A, Sepehrmanesh Z, Ghoreyshi F, Assarian F, Moosavi GA, Saee R, et al. Prevalence of mental disorders in general population of Kashan City. Iranian Journal of Epidemiology. 2010;6(2):16-24
48.Khosravi S. Epidemiology of mental disorders among over 15 years old population in rural and urban area of Borujen, 1994. Journal of Shahrekord University of Medical Sciences. 2003;4(4):31-39
49.The State Council of China. A notification to set up nationwide psychological assistance hotlines against the 2019-nCoV outbreak. Published February 2, 2020. Accessed March 3, 2020. Available from: http://www.gov.cn/xinwen/2020-02/02/content_5473937.htm
50.Van Bortel T, Basnayake A, Wurie F, Jambai M, Koroma AS, Muana AT, et al. Psychosocial effects of an Ebola outbreak at individual, community and international levels. Bulletin of the World Health Organization. 2016;94(3):210-214. DOI: 10.2471/BLT.15.158543
Written By
Robabe Khalili and Leila Karimi
Submitted: June 25th, 2022Reviewed: July 26th, 2022Published: August 24th, 2022