
Abstract
Primary total hip and knee arthroplasty (THA, TKA) are among the most common procedures performed in the United States. The volume of revision TKAs and THAs are also exponentially rising each year. Paramount to the success of total joint arthroplasty (TJA) is the correct choice of biomaterials which are used to reconstruct a particular joint. This chapter explores the history of common arthroplasty biomaterials, their biomechanical properties and current applications. This chapter also discusses modern strategies of improving biomaterial mechanical properties, survivability and sterilisation methods. The contents of this chapter will form an essential resource for practicing orthopaedic surgeons, orthopaedic trainees, researchers and engineers interested in tribology and biomechanics of biomaterials in adult reconstruction.
Keywords
- primary hip arthroplasty
- primary knee arthroplasty
- biomaterials
- alloy
- polymer
- ceramic
- sterilisation
1. Introduction
Primary total hip and knee arthroplasty (THA, TKA) are among the top 5 most common procedures and among the top 5 fastest growing procedures performed across all surgical specialties in the United States [1]. Compared to the available 2014 National Inpatient Sampling figures, the estimated total annual United States use for primary TKA and THA is expected to increase in 2030 and 2040 by 182% and 401% for primary TKA and 129% and 285% for primary THA, respectively [2]. Similarly, projections for revision TKA (rTKA) and THA (rTHA) are estimated to increase from 2014 to 2030 by between 43% and 70% for rTHA and 78% and 182% for rTKAs [3]. Paramount to the success of total joint arthroplasty (TJA) is the correct choice of biomaterials which are used to reconstruct a particular joint.
Biomaterials are defined by the European Society for Biomaterials as “a material that interacts with the biological system to evaluate, treat, reinforce or replace a tissue, organ or function of the organism [4].” In THA and TKA these materials should exhibit a yield stress greater than physiological loading of the joint, while also preventing stress shielding of adjacent bone. These materials should also have an endurance limit which reduces the number of revisions required over a patient’s lifetime, particularly as TJA procedures are increasingly being performed among younger patients [5]. Biomaterials can be considered as being either bioinert, biotolerant or bioactive. Bioinert materials such as ceramics and titanium, do not illicit a biological response from surrounding tissues. Biotolerant materials, such as stainless steel, result in the formation of a fibrous layer due to irritation of surrounding tissues. Bioactive materials, such as hydroxyapatite coatings, result in direct bone on-growth, bonding prosthesis to bone.
The development of orthopaedic biomaterials closely follows the evolution of arthroplasty. Glück used ivory secured with nickel plated screws to replace femoral heads destroyed by tuberculosis in 1891 [6]. Ivory heads were also adapted by Hey-Groves several years later [7]. Delbet developed rubber prosthetic femoral heads in 1919 [8]. Smith-Petersen, in 1932 developed the first mould arthroplasty (Figure 1), which consisted of a hollow glass hemisphere which was fitted over the femoral head to provide a new articular surface [9, 10]. This design was subsequently revised to a Vitallium cup, a cobalt-chromium-molybdenum alloy. Subsequently, during the 1940s and 1950s a plethora of stemmed prosthesis were popularised in an effort to achieve a more anatomic design. Attempts to enhance fixation of these stemmed prostheses resulted in the adoption of dental acrylic cement by both McKee and Haboush in 1953 [11, 12]. Another significant advancement in the field of THA came in the form of articulating prostheses. Wiles popularised the first metal-on-metal THA in 1938, which was among the earliest articulating designs, with both prosthetic femoral and acetabular components [13]. However, poor component stability led to high failure rates, which were later modified by McKee and Ring using varying metal-on-metal prostheses with more reliable fixation methods.
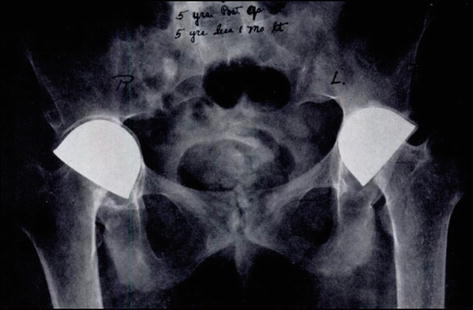
Figure 1.
Smith- Petersen acrylic Mould arthroplasty [
Ultimately, these early designs gave way to the Charnley era in the 1950’s which laid the foundation for modern THA design. Charnley made three major contributions to THA including 1) low friction torque arthroplasty 2) use of polymethylmethacrylate to reliably fix components to bone and 3) the use of high-density polyethylene as a bearing material [6, 14].
A core understanding of the biomaterials used in joint arthroplasty is key to selecting the most appropriate materials for a specific task, patient and type of prosthesis. This chapter provides a practical general overview of modern arthroplasty materials (metal alloys, ceramics, polyethylene and polymethylmethacrylate) rather than an exhaustive description which can be found elsewhere.
2. Metal alloys
The use of metal implants in orthopaedics dates as far back as 1775 with the use of brass wire for fracture osteosynthesis [15]. All metal alloys consist of metals constituted from metallic and non-metallic elements which form a highly organised repeating microstructure. The solvent metal determines the name of the alloy and is considered the base or primary metal. Non-metallic alloying components or solutes, such as oxygen, carbon or nitrogen are added to the base metal, which alters its properties. In their pure form metals tend to have one of three crystalline arrangements. This can be body-centred cubic, face-centred cubic and hexagonal close packed. In the FCC arrangement each atom is in contact with 8 other atoms. Whereas in the BCC and HCP arrangement each atom is in contact with 12 other atoms. During alloy formation, when a molten mixture undergoes solidification, the alloying components substitute for atoms of the base metal in the crystalline arrangement. The size of the non-metallic alloying elements relative to the size of the metallic elements determine the alloy crystal arrangement. If the non-metallic and metallic atoms are of similar size a substitutional alloy is formed, whereby non-metallic elements substitute for metallic elements in the crystalline arrangement, such as brass. If the non-metallic atoms are smaller than the metallic atoms on the other hand then an interstitial alloy is formed, whereby non-metallic atoms occupy spaces in the crystalline structure, such as stainless steel.
The above metallic alloy crystals, group together to form clusters of crystals termed grains. Grains are imperfectly aligned with each other creating gaps between adjacent grains, termed grain boundaries. Microstructure defects such as grain boundaries as well as dislocations and vacancies can all act to increase the propensity for alloy failure. Macrostructure defects, such as scratches and voids can also be a focus for stress and precipitating failure. Several processing methods have been introduced to address these defects including cold and hot working, powder metallurgy techniques to reduce grain size, precipitation hardening and thermomechanical processing.
Metals are susceptible to chemical wear, which is typically the result of corrosion from reactions with the surrounding aqueous physiologic environment [16]. Corrosion is the undesirable dissolution of metal in a solution. This occurs through the formation of an anode and cathode, resulting in metal cation ejection. Typically, passivity through the formation of a thin oxide film on certain metals serves as a kinetic protective barrier. In arthroplasty implant modularity, which results in relative motion between two materials can disrupt the passive oxide layer, resulting in dissolution of metal particles, which is termed fretting corrosion. This has resulted in modular components falling out of favour in primary THRs. Other types of mechanically assisted corrosion such as pitting and crevice corrosion, result in the formation of localised defects and the formation of a stress riser. While implant longevity is a concern, the local and systemic effects of corrosion must also be considered. Therefore, knowledge of the relative corrosion resistance of various metal alloys is essential in TJA, to ensure that they are employed correctly.
Metal alloys with relevance to TJA fall into three main groups 1) stainless steel 2) alloys based on the Cobalt-Chrome (Co-Cr) system and 3) Titanium and its alloys, which will be discussed in this section.
2.1 Stainless steel
Stainless steel was first used in orthopaedic implants in 1926 [17]. Later, Charnley and the Exeter group employed stainless steel for their femoral stems (Figure 2). An iron-based alloy, the stainless steel used in orthopaedic implants is austenitic American Iron and Steel Institute (AISI) 316 L. The number 300 indicates that it is a member of the 300 series of austenitic steel. Austenite steel denotes an FCC crystalline arrangement, with a solid solution of carbon in a nonmagnetic form of iron, which is stable at high temperatures. The FFC structure increases susceptibility to plastic deformation. The alloy includes 3% molybdenum, which increases resistance to pitting and 16% nickel which stabilises the austenitic structure, improving ductility and reducing the alloy’s yield stress. The letter ‘L’ refers to the low carbon content of <0.03% which improves corrosion resistance by reducing sensitisation, a process which results in carbide formation in grain boundaries.

Figure 2.
Exeter V40 stainless steel femoral stem.
Furthermore, the addition of chromium to stainless steel results in the formation of a thin chromium oxide layer (Cr2O3), a process termed passivation which shields the alloy from corrosion. Despite these properties, stainless steel remains susceptible to stress and crevice corrosion. Stress corrosion occurs as a result of exposure to chloride- rich environments whereas crevice corrosion results from the disruption of the passive oxide layer which occurs with undulating deformation.
3. Titanium based alloys
Titanium and titanium-based alloys have been available since the 18th century and are widely used today as biomaterials. They were first applied as a biomaterial in the 1940s in dentistry. However, their mechanical properties and excellent biocompatibility led to them becoming a desirable orthopaedic alloy. Titanium has a low density, high tensile strength and is highly corrosion resistant. The presence of chromium in titanium results in the in vivo formation of a passive oxide layer producing good corrosion resistance. Pure titanium is available in various grades, with the relative oxygen content determining the degree of impurity. Titanium alloy exists as a biphasic structure. As it precipitates from its molten state, an alpha phase results in a HCP arrangement and the beta phase produces a BCC arrangement. This biphasic precipitate results in improved fatigue resistance.
Titanium is commonly alloyed with aluminium, vanadium, niobium, zirconium and tantalum. The most common titanium alloy used in orthopaedics is Ti-6AL-4 V, often termed Titanium 64 due to the 6% aluminium and 4% vanadium concentrations. This alloy possesses a higher ultimate tensile strength than pure titanium and a modulus of elasticity closer to that of bone compared to stainless steel, preventing stress shielding. Additionally, newer generation titanium alloys (TiMoFe, TiMoNbZr and TiNbZrTaSiFe) demonstrate increased elasticity which may improve this capability further [18, 19, 20]. Another, distinct advantage of titanium alloys is MRI compatibility, given that it is non-dielectric and does not rise in temperature when placed in a magnetic field. These properties make titanium an ideal material as an orthopaedic implant. The main disadvantage of titanium, however, is titanium’s poor abrasion resistance and notch sensitivity. Accordingly, titanium is not suitable as a bearing material and should be handled meticulously intraoperatively.
3.1 Cobalt chrome alloy
Cobalt-Chrome (Co-Cr) alloy was introduced into total joint arthroplasty in the early 1900s, as a modification of Vitallium, a common alloy which was in use in dentistry at the time [21]. Most Co-Cr orthopaedic implants contain Cobalt (62–68%), Chromium (27–30%), Molybdenum (5–7%), and Nickel (<2.5%). The alloy was initially used by Smith-Petersen in 1939 in mould arthroplasty and later in the Charnley femoral stem following a move from stainless- steel [9, 22]. Co-Cr possesses several properties which make it a highly suitable alloy for use in arthroplasty. The presence of Cr, as with other alloys, results in the formation of a passive oxide layer providing protection against corrosion, and as a result excellent biocompatibility. Co-Cr alloy has among the highest modulus of elasticity among all commonly used arthroplasty materials. It also possesses a high ultimate tensile strength and has excellent wear resistance.
Modern techniques for implant production use powder metallurgy to reduce the carbon content and thus limit carbide phases which negatively impacts Co-Cr mechanical characteristics. Previous techniques involved cast-wrought production which resulted in increased carbide formation. In contrast, powder metallurgy, involves sieving a fine powder alloy, heating it to a temperature just below melting point before compressing the alloy components in a die cast of the final component shape. Compared to cast-wrought production this method reduces grain size and carbide formation, improving its strength and corrosion resistance.
4. Orthopaedic polymers
4.1 Polyethylene
One of Charnley’s legacy to modern arthroplasty is the introduction of polyethylene as a bearing material for THA [14]. Polyethylene is a linear homopolymer, composed of hydrogen and carbon, represented by the formula ~(CH2-CH2)~. Charnley originally used polytetrafluorethylene, termed Fluron G1 and Fluron G2 manufactured by Imperial Chemical Industries (London, England) as a bearing material for THA due to its low coefficient of friction and biocompatibility [23]. However, poor abrasive characteristics lead to failure of Charnley’s polytetrafluorethylene acetabular cups within 2 years, due to low resistance to creep deformation. Fortuitously, Charnley’s technician, Craven tested a material termed high-molecular- weight polyethylene (HMWPE) which was given to him by a plastic gear salesman. This material was first implanted in 1962 by Charnley when a HMWPE cup was used in combination with acrylic bone cement which was compressed into a reamed acetabulum (Figure 3) [24].

Figure 3.
Charnley hip consisting of HMWPE cup with a Moore stem [
Ultra HMWPE (UHMWPE) is composed of long chains of polymerised alkene, ethylene. It is a semicrystalline polymer, having both a crystalline and amorphous phase. UHMWPE contains a set of ordered crystalline lamellae, with tightly packed randomly orientated macromolecules, embedded in a disordered amorphous phase. UHMWPE consists of up to 200,000 monomers per molecule and a molecular weight ranging from 2 to 6 106 g/mol. Increased molecular weight and degree of cross-bond formation between chains increases the strength and wear resistance of UHMWPE. These properties combined with a low coefficient of friction, resistance to abrasive wear and corrosion, with a high impact strength and toughness have made UHMWPE the arthroplasty bearing material of choice. Comparatively high-density polyethylene has a lower molecular weight (0.05–0.25 106 g/mol) and higher density which results in inferior mechanical properties.
4.1.1 UHMWPE processing
Historically there have been 3 modes of UHMWPE production for orthopaedic implants. Direct moulding involves placing polyethylene powder into a mould of the final configuration of the implant. The powder is then placed under pressure and heated to consolidate it into its final shape. Ram extrusion involves a similar process; however, the powder is fashioned into a cylindrical bar stock which is later machined into the desired final shape of the implant. The final method involves moulding large sheets of polyethylene in which implants are later machined from. A more modern technique has recently been pioneered by Zimmer Biomet termed Hot Isostatic pressing. This process uses high temperature and pressure with argon gas and compression moulding. The process is then completed by a machining operation. These fabrication methods do not significantly alter the physical, chemical or structural properties of the original polymer other than the crystallinity. As the original polyethylene is heated to above melting point, its crystallinity is irreversibly decreased, decreasing fatigue strength. As a result, all polyethylene components possess their original properties prior to sterilisation.
4.1.2 Sterilisation
Polyethylene sterilisation presents a challenge as it cannot be carried out using traditional heating methods due it’s low melting point. The main sterilisation methods used today include high energy radiation (gamma irradiation or electron beam irradiation) or surface treatment. Gamma irradiation is emitted from the decay of a 60Co unstable nucleus whereas electron beam is produced by heating a tungsten filament. Both radiation methods have the advantage of sterilising PE but also causing cross-linking of polymer chains which enhances fatigue strength and wear resistance [26]. However, electron beam irradiation can be performed in a shorter period of time (seconds) and with lower doses of radiation required to achieve a similar degree of crosslinking.
The main disadvantage of high energy radiation is oxidative degradation of the implant through radiolytic bond scission and free- radical generation [27]. Irradiation results in scission of chemical bonds of UHMWPE resulting in free radical formation. Environmental oxygen binds with free radicals permanently breaking the carbon-carbon bonds, a process termed oxidative degradation. This process results in reduced molecular weight and a final component with inferior wear resistance and increased wear debris generation. Macroscopically, oxidative degradation can be seen in retrieved and new components as appearing as a white band or crown effect, which results in severe failure, through delamination and fracture.
Several methods have been employed to reduce the effect of oxidative degradation during irradiation. Manufactures have trialled irradiating PE components in an inert gas such as argon or in a vacuum. Similarly, more sophisticated packaging methods have also become available with particle barrier material, preventing ambient oxygen exposure. Packaging has also been designed to allow the penetration of select gases when chemically sterilised. During the 1990’s, post-irradiation thermal stabilisation melting was also introduced as a means to reduce oxidative degradation by quenching residual free-radicals, allowing them to recombine, improving oxidative resistance. This was initially demonstrated to maintain mechanical property performance standards, but remelting decreased crystallinity, reducing PE fatigue strength.
Subsequently in 2007, UHMWPE stabilisation with antioxidant Vitamin E-diffusion was introduced in the United States [28]. Vitamin E diffusion, limited the need for post-irradiation melting, maintaining PE crystallinity. Synthetic α- tocopherol, the vitamin E used during implant processing, decreases the macro alkyl radicals available to interact with oxygen, inhibiting the ensuing oxidative cascade. Vitamin E can be incorporated into UHMWPE either by post-irradiation vitamin E diffusion or by mixing vitamin E with UHMWPE powder prior to pressurisation. Post-irradiation vitamin E diffusion has the benefit of avoiding the effect of Vitamin E on reducing the number of alkyl radicals available for cross linking but places the cross-linked PE at increased risk of oxidation prior to Vitamin E stabilisation. Mixing Vitamin E with UHMWPE powder has the converse effect.
4.2 Polymethylmethacrylate
The earliest use of acrylic bone cement was by Glück in 1891, for use with an ivory hip prosthesis [6]. However, in 1901 a German chemist, Otto Röhm developed polymethylmethacrylate (PMMA), which is the earliest form of the bone cement which is in widespread use today in orthopaedics [29]. The Judet Brothers developed acrylic femoral hemiarthroplasties prosthesis as a treatment for hip arthritis [30]. However, it was Haboush who was the first to use PMMA as a grout to fix implant to bone [31]. Subsequently, Charnley pioneered to modern use of self-curing PMMA to achieve an implant- bone- cement construct for femoral and acetabular components, in the 1950s and 1960s. Charnley proposed that PMMA, creates an interface between prosthesis and bone to allow for distribution of contact forces and rigid fixation [14, 32]. PMMA acts as a grout which interdigitates with cancellous bone, enhancing interface shear strength. Cement may also act as a shock absorbing layer between elastic bone and a stiff implant with a Young’s modulus (2400 MPa in tension) between cortical and cancellous bone. Cement therefore acts as an elastic interlayer between 2 stiff layers facilitating a more gradual transfer of stress from implant to bone. Currently, cement has a number of orthopaedic applications including; prosthesis fixation, percutaneous vertebroplasty, antibiotic delivery and as an interpositional material for bone defects.
PMMA (C5H8O2) is packaged as 2 separate components; a powdered polymer and a liquid monomer in a 2:1 ratio [33]. The liquid component is supplied as 20mls of fluid, in a brown vial to avoid the deleterious effects of direct sunlight. The liquid monomer contains methyl methacrylate monomer, consisting of microspheres of variable diameter with the size of particles determining the viscosity of the cement. Additionally, heat stable antibiotics may also be added such as gentamicin or vancomycin. Other compounds contained in the liquid component include N,N dimethyl- p toludine (DMPT), hydroquinone, and a colouring agent (e.g green chlorophyl or cobalt blue). The powdered polymers is typically packaged as 40 g of powder containing pre-synthesised PMMA, barium sulphate or zirconium oxide and benzoyl peroxide.
Addition polymerisation of PMMA occurs via an exothermic reaction when the liquid and powdered components are mixed together. Benzoyl peroxide, in the powder component, acts as a catalyst, initiating polymerisation by interacting with DMPT in the liquid component [33]. This interaction liberates free radicals, breaking carbon-carbon bonds within MMA, allowing MMA monomers to couple with the growing polymer chain. Hydroquinone stabilises this reaction, preventing premature polymerisation. The radio-opacifier (barium sulphate or zirconium oxide) and colouring agent (cobalt blue or green chlorophyl) allow for identification of cement, radiologically and intra-operatively.
This chemical reaction is characterised by 4 distinct phases. The mixing phase or sandy stage (phase 1) occurs when powder and liquid components are mixed together (lasting roughly 30s). The waiting phase or sticky phase (phase 2), lasts approximately 1 to 3 minutes (depending on cement viscosity) and ends when the cement will easily separate from a gloved finger. The working phase (phase 3) occurs when the cement can be easily handled and signals when implants can be inserted, lasting approximately 5 minutes for high viscosity cement. The setting or hardening phase (phase 4) lasts approximately 1 minute 30 seconds to 2 minutes for high viscosity cements. These phases are influenced by a number of endogenous and exogenous factors. Increasing environmental temperatures and humidity decreases cement working time. Other factors such as a decreased powder liquid ratio increases setting time. The final biomechanical performance of cement can also be influenced by a number of exogenous factors such as mixing technique, sterilisation methods, antibiotics additives and choice of radio-opacifier.
5. Ceramics
Ceramics were popularised in the 1970’s as bearing materials. Ceramics consist of metallic elements such as aluminium, zirconium and silicon covalently and or ionically bound with non-metallic elements. The main advantage of ceramic bearings is the reduction of wear debris in the periprosthetic space, which can precipitate the osteolysis cascade and aseptic loosening [34] associated with metal-on-metal and metal-on-PE bearing couples. Oxide ceramics used in total joint arthroplasty (TJA) are chemically inert after binding to oxygen, resulting in excellent biocompatibility. Ceramics also possess a low surface roughness and high hardness, possessing the highest modulus of elasticity of any other biomaterial used in TJA.
Unfortunately, the trade-off of high hardness is ceramic bearing brittleness and subsequent catastrophic failure. The first ceramic bearings used in THAs in 1971 were marred by catastrophic failure due to acute debonding at the implant-cement interface of cemented ceramic sockets resulting in aseptic loosening and implant fracture. In more modern systems this has been corrected with the addition of metal backed acetabular shells to ceramic liners [35]. The primary mode of failure, in more modern systems is now edge loading due to implant mispositioning, resulting in stripe wear. This process disrupts the oxide layer, reducing fracture toughness and increasing surface roughness. Microscopic flaws, introduced during the manufacturing process or machining such as notches, pores and scratches can also result in stress concentration, propagation of cracks and subsequent abrupt failure [34].
Ceramics are fabricated by mixing fine ceramic powder and water together and compressing the mixture into casts of the desired final shape. The mixture is then sintered in a kiln to bond the particles together and to increase density before being polished. The resulting organised crystalline microstructure and mechanical characteristics are subsequently determined by the grain size, porosity, crystallinity and density together with the implant design. Ceramics can be classified as non-oxides, oxides and composites, with oxide ceramics the material of choice in THA.
With the increased uptake of ceramic-on-ceramic bearings globally, audible squeaking arose as a new complication, with an incidence between 0 and 24.6% [36]. There have been a number of purported mechanisms described accounting for this complication. Suggested risk factors for COC squeak have included increased stripe wear and disruption of film-fluid lubrication, edge loading due to malposition of the acetabular cup, increased body mass index and femoral stem design geometry, among many others [37].
5.1 Aluminium oxide
Aluminium oxide (Al2O3) was developed as a biomaterial in the 1960’s, making it a well characterised biomaterial. Modern alumina is processed using hot isostatic pressing, a process which reduces inclusions, grain size and grain boundaries, increasing hardness and increasing scratch resistance. Alumina also possesses a very low coefficient of friction due to a low surface roughness, resulting from its low grain size. This excellent tribological performance is further compounded by alumina’ s high wettability and resulting film-fluid lubrication, which reduces in vitro wear. Retrieval studies have demonstrated alumina-on-alumina wear rates of a few micros per year [38]. Biologically the typical response to alumina wear debris is fibrocytic with no giant cell formation and little induction of macrophages, reducing osteolysis [35]. The estimated lifetime risk of catastrophic failure of alumina femoral heads is estimated to be 0.004% [38].
5.2 Oxidised zirconium (zirconia)
Oxidised zirconium (ZrO2) is a ceramic composite bearing which was introduced as a means to reduce the catastrophic failure rates associated with alumina heads, while still also retaining the desirable wear characteristics of smaller femoral heads on polyethylene [34]. Pure zirconia is not used as a bearing material as it undergoes phase transformation between its three crystalline arrangements (monoclinic, cubic, tetragonal). This can result in volume and shape changes that increase the susceptibility to fracture. As a result, pure zirconia, requires stabilisation through a process known as transformation toughening. Zirconia can be stabilised with CaO, Y2O3 or MgO which controls phase transformations.
Zirconia toughened alumina (ZTA), is a composite which consists of zirconia dispersed in an alumina matrix (Figure 4). This modification resulted in the improved strength, fracture toughness and tensile strength compared to aluminium oxide [34]. ZTA can be strengthened further by the addition of Cr2O3 and SrO, which prevents crack propagation.

Figure 4.
BIOLOX Delta composite ceramic femoral head containing Aluminium oxide, zirconia and strontium oxide [
6. Summary
The responsibility of choosing the correct biomaterial in TJA lies solely with the operating surgeon. Surgeons should have a good working knowledge of the properties of commonly implanted biomaterials and should regularly scrutinise joint registry data when determining the most suitable biomaterial according to its intended use, in order to optimise patient outcomes.
References
- 1.
McDermott KW, Freeman WJ, Elixhauser A. Overview of operating room procedures during inpatient stays in US hospitals, 2014: statistical brief# 233. 2018 - 2.
Singh JA, Yu S, Chen L, Cleveland JD. Rates of total joint replacement in the United States: Future projections to 2020-2040 using the national inpatient sample. The Journal of Rheumatology. 2019; 46 (9):1134-1140 - 3.
Schwartz AM, Farley KX, Guild GN, Bradbury TL Jr. Projections and epidemiology of revision hip and knee arthroplasty in the United States to 2030. The Journal of Arthroplasty. 2020; 35 (6):S79-S85 - 4.
Williams DF. Definitions in Biomaterials: Proceedings of a Consensus Conference of the European Society for Biomaterials. Chester, England: Elsevier Science Limited; 1986. p. 1987 - 5.
Ravi B, Croxford R, Reichmann WM, Losina E, Katz JN, Hawker GA. The changing demographics of total joint arthroplasty recipients in the United States and Ontario from 2001 to 2007. Best Practice & Research Clinical Rheumatology. 2012; 26 (5):637-647 - 6.
Learmonth ID, Young C, Rorabeck C. The operation of the century: Total hip replacement. The Lancet. 2007; 370 (9597):1508-1519 - 7.
Groves EWH. Some contributions to the reconstructive surgery of the hip. Journal of British Surgery. 1927; 14 (55):486-517 - 8.
Gomez PF, Morcuende JA. Early attempts at hip arthroplasty: 1700s to 1950s. The Iowa Orthopaedic Journal. 2005; 25 :25 - 9.
Smith-Petersen M. Evolution of mould arthroplasty of the hip joint. The Journal of Bone and Joint Surgery British Volume. 1948; 30 (1):59-75 - 10.
Knight SR, Aujla R, Biswas SP. Total hip arthroplasty-over 100 years of operative history. Orthopedic Reviews. 2011; 3 (2):72-74 - 11.
McKee G. Total hip replacement—Past, present and future. Biomaterials. 1982; 3 (3):130-135 - 12.
McKee G, Watson-Farrar J. Replacement of arthritic hips by the McKee-Farrar prosthesis. The Journal of Bone and Joint Surgery British Volume. 1966; 48 (2):245-259 - 13.
Wiles P. The surgery of the osteo-arthritic hip. British Journal of Surgery. 1958; 45 (193):488-497 - 14.
Charnley J. Arthroplasty of the hip: A new operation. Clinical Orthopaedics and Related Research®. 1973; 95 :4-8 - 15.
Hernigou P, Pariat J. History of internal fixation (part 1): Early developments with wires and plates before world war II. International Orthopaedics. 2017; 41 (6):1273-1283 - 16.
Jacobs JJ, Gilbert JL, Urban RM. Current concepts review-corrosion of metal orthopaedic implants. JBJS. 1998; 80 (2):268-282 - 17.
Li B, Webster T. Orthopedic Biomaterials: Progress in Biology, Manufacturing, and Industry Perspectives: Springer; 2018. pp. 175-195 - 18.
Abdelrhman Y, Gepreel MA-H, Kobayashi S, Okano S, Okamoto T. Biocompatibility of new low-cost (α+ β)-type Ti-Mo-Fe alloys for long-term implantation. Materials Science and Engineering: C. 2019; 99 :552-562 - 19.
Nnamchi PS, Obayi C, Todd I, Rainforth M. Mechanical and electrochemical characterisation of new Ti–Mo–Nb–Zr alloys for biomedical applications. Journal of the Mechanical Behavior of Biomedical Materials. 2016; 60 :68-77 - 20.
Kopova I, Stráský J, Harcuba P, Landa M, Janeček M, Bačákova L. Newly developed Ti–Nb–Zr–Ta–Si–Fe biomedical beta titanium alloys with increased strength and enhanced biocompatibility. Materials Science and Engineering: C. 2016; 60 :230-238 - 21.
Callaghan JJ, Rosenberg AG, Rubash HE, Clohisy JC, Beaulé PE, Della Valle CJ. The Adult Hip: Hip Arthroplasty Surgery. United States: Wolters Kluwer Health Adis (ESP); 2015 - 22.
Smith-Petersen M, Larson CB, Aufranc OE, Law WA. Complications of old fractures of the neck of the femur results of treatment by vitallium-mold arthroplasty. JBJS. 1947; 29 (1):41-46 - 23.
Li S, Burstein AH. Ultra-high molecular weight polyethylene. The material and its use in total joint implants. JBJS. 1994; 76 (7):1080-1090 - 24.
Charnley J. The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. The Journal of Bone and Joint Surgery British volume. 1972; 54 (1):61-76 - 25.
Jackson J. Father of the modern hip replacement: Professor sir John Charnley (1911-82). Journal of Medical Biography. 2011; 19 (4):151-156 - 26.
Grobbelaar C, Du Plessis T, Marais F. The radiation improvement of polyethylene prostheses. A preliminary study. The Journal of Bone and Joint Surgery British volume. 1978; 60 (3):370-374 - 27.
Sobieraj M, Rimnac C. Ultra high molecular weight polyethylene: Mechanics, morphology, and clinical behavior. Journal of the Mechanical Behavior of Biomedical Materials. 2009; 2 (5):433-443 - 28.
Oral E, Wannomae KK, Rowell SL, Muratoglu OK. Diffusion of vitamin E in ultra-high molecular weight polyethylene. Biomaterials. 2007; 28 (35):5225-5237 - 29.
Rohm O. On the Polymerization Products of Acrylic Acid. Chemistry (dissertation). Tubingen: University of Tubingen; 1901 - 30.
Judet J, Judet R. The use of an artificial femoral head for arthroplasty of the hip joint. The Journal of bone and joint surgery British volume. 1950; 32 (2):166-173 - 31.
Haboush E. A new operation for arthroplasty of the hip based on biomechanics, photoelasticity, fast-setting dental acrylic and other considerations. Bulletin of the Hospital for Diseases Orthopaedic Institute. 1953; 14 :242-277 - 32.
Charnley J, Charnley J. Acrylic Cement in Orthopedic Surgery Baltimore. Philadelphia, PA, USA: The Williams and Wilkins Co; 1970. p. 36 - 33.
Jaeblon T. Polymethylmethacrylate: Properties and contemporary uses in orthopaedics. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2010; 18 (5):297-305 - 34.
Bal B, Garino J, Ries M, Rahaman M. A review of ceramic bearing materials in total joint arthroplasty. Hip International. 2007; 17 (1):21-30 - 35.
Hannouche D, Hamadouche M, Nizard R, Bizot P, Meunier A, Sedel L. Ceramics in total hip replacement. Clinical Orthopaedics and Related Research®. 2005; 430 :62-71 - 36.
Owen D, Russell N, Smith P, Walter W. An estimation of the incidence of squeaking and revision surgery for squeaking in ceramic-on-ceramic total hip replacement: A meta-analysis and report from the Australian Orthopaedic Association National Joint Registry. The Bone & Joint Journal. 2014; 96 (2):181-187 - 37.
Currier JH, Anderson DE, Van Citters DW. A proposed mechanism for squeaking of ceramic-on-ceramic hips. Wear. 2010; 269 (11-12):782-789 - 38.
Willmann G. Ceramic femoral head retrieval data. Clinical Orthopaedics and Related Research®. 2000; 379 :22-28 - 39.
Exactech Inc. BIOLOX Delta Ceramic Femoral Head | Total Hip Arthroplasty. 2022. Available from: www.exac.com