
Abstract
People living with Alzheimer’s disease and related dementias (PwADRD)experience declined memory, language, problem-solving and other cognitive functions caused by the disease. They face major challenges in self-care and assistive living, including equitable access to assistive technology and care, the right to choose where to live, protection of privacy and security, and the preserving their personhood and social connections. Fast advances in telecommunication, Internet of Things (IoT) technology, and artificial intelligence make it possible to devise an assistive technology ecosystem to address these challenges. This chapter presents an assistive technology ecosystem that enables autonomy, independence and interdependence among PwADRD, their circle of care and society. Participatory action research and design methodology underpin this ecosystem’s design and implementation. We also discuss funding policy and health system changes needed to facilitate the affordability and sustainability of such an ecosystem and, ultimately, to empower PwADRD and their caregivers to have a meaningful quality of life.
Keywords
- assistive technology ecosystem
- people living with Alzheimer’s disease
- dementia
- participatory action research design
- self-care
- independent living
- interdependence
- IoT
- artificial intelligence
1. Introduction
Alzheimer’s disease and related dementia (ADRD) is an acquired cognitive disorder that causes a person’s progressive decline in memory, language, learning, problem-solving and other cognitive skills [1]. Alzheimer’s disease is the leading cause of dementia, with a larger prevalence in women and older adults - 72% of people with Alzheimer’s are projected to be women by 2030; most individuals who are diagnosed with ADRD are 65 or older, and after the age of 65, the risk of ADRD doubles every 5 years, reaching nearly one-third at age 85 [2]. According to the World Health Organization, approximately 55 million people around the world currently live with dementia. In 2022, 10 million new cases of dementia were reported around the world [1]. In Canada, approximately 570,000 people over the age of 65 currently live with dementia. In addition, approximately 124,000 people were recently diagnosed with the syndrome [2]. These numbers are rising sharply owing to increased life expectancy globally as well as earlier diagnoses. In 2015, about 15% of Canadians were 65 or older; and by 2030, one in four Canadians will be an older adult [3]. This translates into an unprecedented number of people living with ADRD (PwADRD) with a relatively small number of people to support them.
PwADRD experiences a progressive decline in cognitive functions and sudden changes in mood and behavior. These changes affect a person’s ability to perform everyday activities. PwADRD experience challenges with self-care, limiting their ability to perform or complete activities of daily living themselves. This led to additional caregiving demands on family members and personal care workers who provide care and support for those living in their own homes or congregate settings. As of 2020, ADRD is among the top four diseases from the standpoint of global healthcare pressure points and is anticipated to be in the top three by 2030 [4]. In Canada, a recent study estimates that the combined Canadian healthcare costs and out-of-pocket caregiver costs from ADRD amounted to $10.4 billion in 2016; by 2031, this Figure is expected to increase to $16.6 billion [4]. The alternative of living in a residential facility is both very costly and unsustainable, which can expose PwADRD to severe health risks (as exemplified in the COVID-19 pandemic). In Ontario, the cost of memory care (a facility providing specialized care for those living with dementia) is $4000–$6500 per month per person [5]. There is a first-ever Canadian Dementia Strategy in Canada that has called for a shift to provide integrated community-based care as the primary means of supporting PwADRD and their care partners in Canada [6]. However, for a community-based system to be successful, the health and well-being of both PwADRD and their care partners must be properly supported [7].
Technological advances make it possible to devise an IoT ecosystem to address self-care-related challenges while simultaneously improving the quality of life of PwADRD and their care partners and mitigating the global economic burden [6, 8]. While some disparate IoT solutions have been developed across the globe by research groups such as those associated with the Active Assisted Living (AAL) Programme (http://www.aal-europe.eu/) and AGE-WELL (https://agewell-nce.ca/), a single ecosystem that can support the implementation of assistive technologies at scale is still lacking for PwADRD in their chosen dwelling, particularly at their own home. Furthermore, interoperability, data-sharing, and privacy and security are identified as major challenges in AAL.
2. The voice of the users – participatory action design methodology
Participatory Action Research is an innovative research design which can be implemented when developing resources for PwADRD. The qualitative research methodology is collaborative between researchers and participants [9]. This approach is effective in addressing stigma related to dementia by engaging members of the community to take action and inspire and empower social change [10]. A participatory design implements a community-based approach to planning and executing research studies. The partnership between the researchers and the community is essential when experimenting with assistive technologies for use by individuals with dementia. Tierson and colleagues found that implementing a participatory action research design enhanced their understanding of the experiences lived by PwADRD [11]. Furthermore, Goeman et al. found that the researchers benefitted from the high level of social interactions with PwADRD [12]. Through this engagement, the researchers developed greater insights into the needs of PwADRD and their caregivers. The studies demonstrate that the inclusion of PwADRD enabled researchers to receive first-hand, instantaneous feedback from the stakeholders who would benefit from their findings. Hence, this research approach leads to input from PwADRD based on their real-life experiences using the technologies. Overall, it facilitates the development of more effective products and services for PwADRD.
When developing participatory designs, it is important to recognize the challenges faced by researchers when considering the progressive cognitive decline experienced by PwADRD. Researchers may also experience challenges building strong relationships with the local community [13]. In addition, there is also a level of difficulty experienced by PwADRD in communicating feedback on the pilot technology. This may pose an additional challenge for the researcher in identifying potential user needs. However, best practices can be implemented to mitigate these challenges. Using a community-based approach, researchers may consider incorporating innovations such as AI technologies or personas to assist PwADRD in communicating their feedback. An additional example may include visual aids to help create familiar environments and enhance an individual’s ability to recall past events. These approaches demonstrate the inclusive nature of participatory design when experimenting with assistive technologies [14]. This research approach leads to a strengthened network between PwADRD, researchers, and technology developers.
3. Independence and interdependence in active assistive living
In this section, we argue that health can only be understood in a relational context. Robinson Crusoe, living alone on his desert island, might have the most desirable and healthy physique. However, his loneliness and lack of human interaction meant he was healthy in only the narrowest sense. Human identity is found in our relationship with others, from the beginning to the end and beyond – in the memories we have and other legacies we leave. The division between ‘you’ and ‘me’ in these caring relationships becomes diminished. The vulnerability of one becomes the vulnerability of others; the disability of the one becomes the disability of the other [15]. The definition of independence by the healthcare system focuses on individuals and an individual’s performance capacity [16]. While the independence of PwADRD is an important and measurable outcome of any intervention, we also argue that Assistive Technology (AT) should focus on advancing the interdependence of people with disabilities. This has been challenged by activists and scholars within and outside the AT community [17]. There is increasing recognition of the importance of social and cultural factors in AT use and growing evidence that social relationships can enable PwADRD to lead meaningful lives and improve the well-being of their caregivers [17, 18]. Therefore, “independence” is no longer suffice as the primary goal of AT design. Researchers have proposed approaching AT design through a comprehensive holistic lens, considering individuals’ autonomy, independence, and interdependence in the AT ecosystem [17].
Autonomy describes one’s ability to make decisions on behalf of self and refers to one’s individuality, dignity, integrity, responsivity, and self-knowledge [16]. Autonomy as a human right is considered a fundamental ethical principle of healthcare and is generally valued by the individual [19]. Autonomy does not stop at the individual level, as one’s choices are influenced by their development, family and social networks, and spirituality [16]. Recent research has also shown the importance of autonomy to PwADRD with increasing self-advocacy for participation and choice in decisions regarding their care [19]. Independence describes one’s ability to perform tasks and activities and is often a key goal for healthcare interventions in Western culture [19]. This emphasis on independence places value on self-reliance, discouraging individuals from reaching out to others for help, which in some cases, can be a key factor in allowing individuals to stay within their homes and communities. Interdependence is the interconnectivity of individuals with each other and with their environments. Lindemann suggests that interdependence is a natural part of community living: “
The latest research suggests that interdependence can create new opportunities in AT research and development in crowd work, ability-based design, and navigation [17]. An interdependence lens can also expand ability-based design and navigation research by incorporating features that adapt to different social contexts and relations. It allows people to reduce the barriers created by their disabilities through collaboration with others and by relying on each other’s strengths. By employing the participatory action methodology introduced in the previous section, AT design pays attention to the relations between people and technologies, individuals’ dual roles as recipients and contributors to AT and systemic bias. Participatory action methodology sheds light on the transient nature of interdependence and the fluid nature of disability [14]. By understanding that accessibility depends on factors specific to a situation, AT design can account for individual experiences and uncover a broader range of influential factors. The traditional view of people with disabilities as only recipients of support constantly undervalues their contribution to the advancement of accessibility for all. Interdependence encourages researchers and developers to assess relations between people without AT to identify potential biases and support more meaningful access. For example, observations of how blind and sighted partners navigated new environments revealed challenges due to navigation research informed by misconceptions of blind navigation held by sighted people. Additionally, interdependence suggests the possibility of simultaneous relations influencing the accessibility of a particular situation, where people receiving access may also be providing it. By viewing access as an ongoing process where people offer and receive access from each other, AT design can better understand the duality of each participant’s role. Interdependence considers all participants being mutually reliant, thus bringing our focus to engaging people with disabilities to co-create accessibility solutions. In addition, society has traditionally considered the actions and contributions of people with disabilities as less important. It fails to recognize the efforts required to navigate complex insurance and funding programs and specialized technology interfaces. Interdependence addresses the systemic undermining of people with disabilities by assuming all participants as crucial to the relationship, resulting in designs that challenge ability-based hierarchies. For example, Incloodle features a cooperative photography application that supports equal participation of neuro-typical and neuro-divergent children [21].
The following section presents an IoT ecosystem that enables active assistive living for PwADRD. Autonomy, independence and interdependence are the underlining principles of this ecosystem.
4. Active assistive living IoT ecosystem
Currently, the state-of-the-art in care for PwADRD involves self-care with the support of care partners who may be: (i) healthcare support workers either at home or in an assisted living facility; or (ii) family and friends. In both cases, there are opportunities to use AT to support autonomy, independence and interdependence, provide a better quality of life and control rapidly increasing costs. Although there are integrated digital solutions at major urban research hospitals for post-operative care, and multiple apps for self-care, there are no ecosystem solutions that are secure, energy-efficient and user-friendly for most Canadians with self-care needs.
We propose a first-of-its-kind suite of IoT devices and associated ecosystems optimized to support the independence of PwADRD. The system, as conceived, supports PwADRD in current best practices such as: “
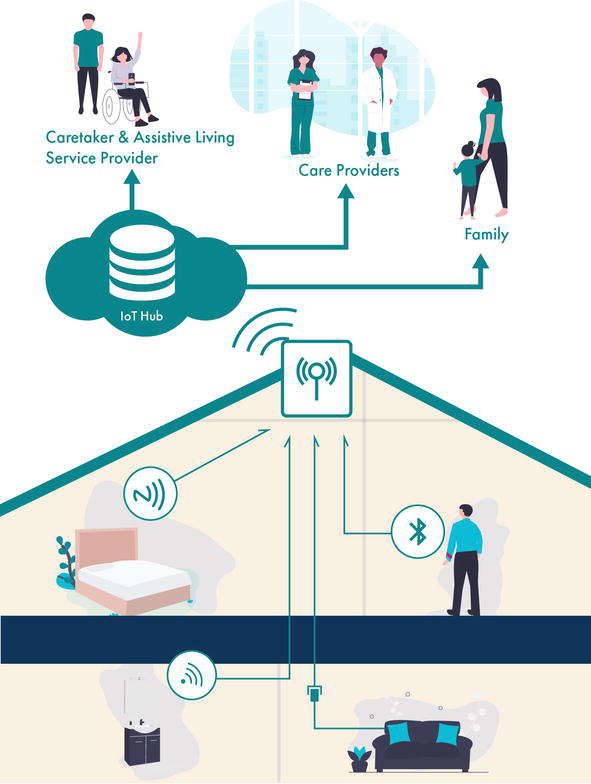
Figure 1.
IoT ecosystem enabling self-care.
4.1 IoT ecosystem and integration
A key challenge with a person-centric technology is that it often requires custom deployment for individuals. This makes the ecosystem static and unable to adapt to disease progression or a person’s changing circumstances. An PwADRD can go through several transitions as the condition progresses, experiencing mild decline early on to more severe challenges later in the disease trajectory. The individual can also experience day-to-day and even within—day variations in symptoms. The proposed ecosystem seeks to address this explicitly by providing the capability to continuously learn the progression of the disease and adapt and extend mechanisms to address concerns in a non-intrusive manner while documenting the trajectory and day-to-day patterns for healthcare providers for care and evidentiary purposes.
The ecosystem consists of hardware and software components. The hardware is comprised of heterogeneous IoT devices, intelligent routers that integrate these devices, and a heterogeneous processing platform. The software components include integration software within the person’s home, implementations of learning algorithms to provide self-adaptation, and service-related software to use the cloud as well as exchange sensitive information with health service providers and other care partners. These components can be further categorized into the following roles and responsibilities: (1) IoT devices that sense important information about the person’s interaction with their environment; (2) processing platforms that allow for processing of the sensed information and automatic recommendations based on sensor data; and, (3) use of an integrated service for automated analysis and monitoring through which care partners and the ecosystem interact with each other. The system also needs to allow users flexibility as to how their data is used and shared.
The IoT devices include the proposed devices mentioned above, and devices that are currently available in the market. For example, door and motion sensors are key to addressing concerns related to navigating surroundings and getting lost. These sensors provide information that the processing platform uses to execute learning algorithms to determine whether the initial care plan constructed by care partners is helpful to the person, and if not, then adjustments are dynamically proposed. Certain personalization and adjustments of the caregiving plan can be automatically deployed, but some require authorization. This authorization would be enabled via the integrated service system, where the suggested adjustments are communicated to the care partners who approve them before the ecosystem seamlessly alters the deployment software. Note that this would require limited physical intervention from the care partner. Consider a user whose disease progresses over time where initially the user could operate the stove without any assistance but gradually requires reminders and at more advanced stages, needs automated turn-off capabilities. During early stages, the care plan may want the user to be independent and operate the stove themself; hence, the sensor only monitors that the stove is turned off when the user is not near the stove for an extended period of time. However, when the learning algorithms identify several instances where the user has forgotten to turn off the stove, automatic reminders could be sent via the ecosystem. In such situations, care partner intervention may not be required. At later stages, the functionality of the ecosystem will adapt according to a person’s progression of the disease and the availability of care resources in the circle of care. The proposed approach addresses the need to provide accurate indicators of disease progression to the care providers and the timely adaptability of a person-centred care plan, particularly in terms of self-care at home.
4.2 IoT device research
This IoT ecosystem requires a heterogeneous mix of portable and wearable IoT devices. By leveraging existing circuit and system technologies wherever possible, focus can be placed on security, ecosystem integration, and energy management aspects that are crucial to IoT device deployment in a field trial. IoT devices applied to self-care are typically powered by a battery that imposes strict constraints on performance and the quality and duration of service. We need to improve the energy efficiency of existing technologies by modifying key circuit functions that harvest energy and extend IoT devices’ battery and service life for low data rate (i.e., 1-100kbit/s) ADRD applications outlined herein. The first improvement is a solar antenna (sol-ant) capable of harvesting light (from the solar cell) and microwave energies (from the antenna) simultaneously [23]. The second augmentation is energy harvesting, storage and delivery via a power management sub-system that extends battery and service lifetimes substantially.
A block diagram of the proposed autonomous wireless system is shown in Figure 2. It consists of a wireless transceiver, baseband signal processing circuits, embedded memory, a microcontroller, power management, and CMOS sensors. Autonomy for the wireless system reduces maintenance (e.g., battery charging, replacement). The wireless transceiver shares information collected by the CMOS sensors with smartphones, wireless hotspots, and sensor nodes in the ADRD ecosystem. The goal is to build an autonomous wireless system leveraging existing commercial technologies augmented by the solar and power management sub-systems. Energy harvested continuously by the solar can be stored on a supercapacitor or used to recharge a button-cell battery. The transceiver uses the button cell as a start-up power source, extending its operating lifetime to 3–5 years. Poor energy efficiency reduces operational lifetime and increases battery size, which is undesirable in the ADRD application. If a continuous operating of 50 days from a 10-gram Li- ion button-cell battery (i.e., 120 W-h/kg energy density) is desired, a transceiver (Tx/Rx) energy efficiency below 10 nJ/bit is required, i.e., 10x better than conventional technologies such as WiFi, Bluetooth or Zigbee. The aim is to extend the service time of the wireless transceiver operating at 1-100kbit/s, and push efficiency below 10 nJ/bit by harvesting energy from multiple sources using the autonomous power management system. Sources of energy available in a typical home are: light, thermal, mechanical vibration, and radio-frequency (RF) energies.
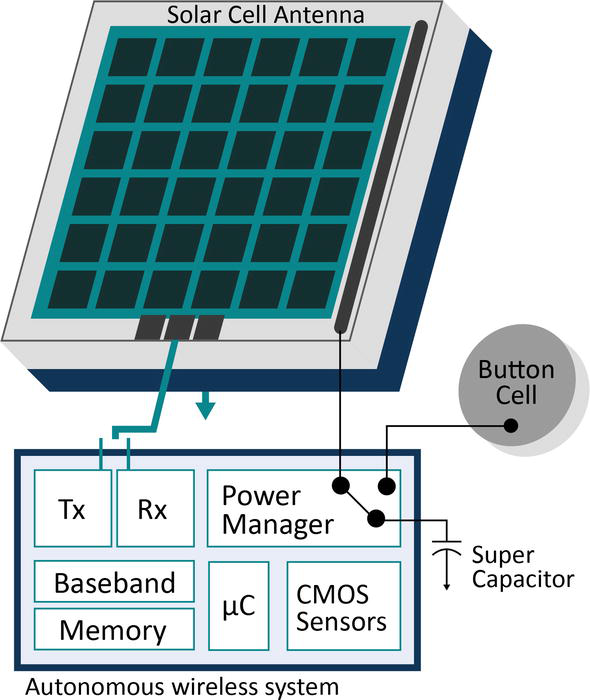
Figure 2.
Block diagram of the proposed autonomous wireless system.
A photovoltaic solar cell antenna (solant) capable of harvesting light and RF energies are capable of generating more energy from a surface area of just a few cm2 when operating indoors than other methods [24]. Unfortunately, solar and other renewable energy sources are intermittent. Therefore, energy harvested from the solant must be stored on a high-density supercapacitor and in a rechargeable button battery via a charge pump. The 1-Farad supercapacitor stores enough energy from the solant to bridge peaks in energy demand from the wireless transceiver. Energy from the battery initially bootstraps the power management sub-system system (i.e., ‘cold start’ when the supercapacitor is discharged). A DC-DC converter draws energy from the supercapacitor to operate the wireless transceiver, sensor interface, and digital circuitry when required. It converts a voltage ranging from 0.6–2.75 V to a regulated 0.9 V supply for the CMOS transceiver. The power consumption of digital and memory circuits has an exponential relationship with the supply voltage. It makes sense to lower the voltage and reduce the power consumption. It is attractive for large memories where the leakage power is high. However, a simple voltage reduction is not without its challenges. The memory access time is increased significantly with reduced voltage. In addition, the memories’ ability to retain data is also reduced linearly with the voltage reduction. Data retention is further eroded due to manufacturing variations in advanced technologies. Recent research demonstrated memories and digital circuits working at 250–300 mV range for low-power and low-energy applications [24, 25]. However, additional investigation is needed for ultra low-voltage (less than 200 mV) digital and memory circuits to further enhance power and energy efficiency to extend the battery life.
4.3 Safety, security, privacy and trust considerations
Security and privacy are arguably the most important attributes that must be provided at the level of the ecosystem rather than for components only. Of course, the ecosystem is a composition of those components; thus, the security and privacy of and from components are necessary but not sufficient for the system as a whole. Systems security and privacy are well known to be significant technical challenges in any system of reasonable scale and complexity. Challenges can be categorized as (1) Security of individual components and privacy protection of data within individual devices, (2) Security of the human users from the system, (3) Security of the system, i.e., the composition of the individual components, (4) the privacy the system provides to the data both at rest and in transit and (5) the ability for users to make informed choices regarding privacy and system use. Towards (1), considerable work has already been done on both tamper-resistance of devices and the security and privacy such devices provide [26, 27]. The technique in this regard is to carefully isolate data and components that need to be trusted from those that do not and enclose the former using, for example, tamper-resistant screws to preclude physical access, and also hardware-enforced isolation built into the. Cutting-edge techniques such as lightweight cryptography can ease computation and communication overhead and yet provide adequate security guarantees [28].
Towards (2), a necessary design constraint is obtaining consent. The design and engineering of the system, particularly its usability aspects, must (a) clearly solicit user-consent, and, (b) do so in a simple, intuitive manner from the standpoint of Human Computer Interaction [29, 30, 31]. Towards (3), it is well-established in the field that the composition of two secure systems is not necessarily secure. Consequently, sound techniques for secure composition are required. Towards (4), compliance with privacy legislation, specifically the Personal Information Protection and Electronic Documents Act (PIPEDA), as well as with the corresponding US Health Insurance Portability and Accountability Act (HIPAA), will be critical. Properties such legislation requires will be encoded precisely in a manner that can then argue strongly, or even prove, that they have been met. Regarding (5), developing and implementing an at-home monitoring system has a multitude of complex ethical challenges regarding understanding what the system does and being able to make informed choices on what and when information is used. This open problem has remained a significant barrier to the uptake and use of these types of systems. Participatory action research with PwADRD and their care partners can be used to create new ways of supporting informed consent. This can be supplemented by the progressive information and permissions paradigm that is currently used and familiar to people living with dementia as an underlying framework [32, 33, 34].
The shift from deploying sets of devices to a secure learning ecosystem represents a major advent in technology and system thinking. Attention to minimizing energy needs and making the system cost-effective are essential in making the system sustainable and affordable on a large scale. The ability to help individuals stay longer in their own homes and delay the shift to a care facility as long as possible will benefit their quality of life and make the best use of scarce economic resources. Currently, waiting lists for long-term care are long, and the dangers of the rapid spread of infection in these facilities are apparent. Although the application here is to ADRD, the ecosystem could also be applied to other areas of healthcare where monitoring of persons could be beneficial.
4.4 General purpose technology in the assistive technology ecosystem
Our society has generally become more inclusive. As a result, many technologies designed for the general population have embedded functions to be used as assistive technology. The Association for Advancement of Assistive Technology in Europe (AAATE) has identified the convergence of general purpose (i.e. mainstream) technology and assistive technology as an ongoing trend where products will offer more comprehensive ranges of functions that can benefit a larger portion of the population [35]. An example of this trend is the replacement of disability-specific electronic aids to daily living with mainstream smart home technologies such as Google Home and Amazon Echo. As technology design continues to focus on adaptability and flexibility, mainstream technologies will provide more affordable and better options for people with disabilities to access features that would traditionally only be available in assistive technologies. Using mainstream technologies in the IoT ecosystem presented in this chapter also has the potential to save costs and reduce resource demands of the healthcare system, thus significantly improving the ecosystem’s sustainability. This has been demonstrated in a study conducted by the Centre for International Research on Care, Labour and Equalities in England [35]. Other studies highlighted the potential of mainstream technology to support people’s care without damaging their sense of self [36]. It is reported that the participant prefers mainstream technologies as they are perceived as commonplace and a part of everyday life. This study also identified the need to understand their contribution to social isolation and cautioned against underestimating the demand for Wraparound services [36].
5. Systematic changes
Inevitably, the cost is a barrier to AT adoption. In Canada, healthcare is mainly the province’s responsibility, and variations in funding mechanisms, eligibility criteria, types of funded devices, and extend of funding exist across provinces [37]. Within each province, based on the type of recipient and the program for which they are seeking support, funding may come from federal and provincial programs, private insurance, charity programs, foundational grants, and donations. The lack of a holistic approach between funding sources makes it difficult for a PwADRD to navigate the funding system, resulting in service gaps where groups need AT without financial support. Restrictive eligibility criteria can further limit access by increasing an individual’s burden to demonstrate financial and AT needs. Specific functional disabilities may limit entitlement, leaving more generalized AT or AT not related to the specific disability inaccessible, even if they have the potential to improve the user’s overall quality of life.
These challenges are compounded by variations in eligible device types and considerations for customization, maintenance, repair, and replacement. Certain programs require the technology to have been on the market for a minimum of 1 year before it is approved for funding [37]. Other programs may look at the context of how the AT is to be deployed and will only supply AT as part of a package to meet a specific need. Funding for general-use technologies is also inconsistent between programs, with some promoting the use of consumer products while others exclude these from consideration. To further complicate the issue, some programs will support custom build and upgraded solutions, while others only fund basic models, with applicants having to pay out of pocket for any upgrades. Lastly, programs may only fund AT that supports essential daily living activities and limit their access to leisure purposes. There is also little consideration for user training for fully utilizing the AT they have received. Some programs will provide education and training support, but many consider the device as a one-time expense with minimum funding for Wrap around services. The treatment of AT access as isolated events can also create challenges as an individual’s situation changes, triggering a need for reassessment of their AT needs. Without a funding mechanism to support ongoing evaluation, the impact of funding programs may be limited.
A holistic approach will be essential for various programs to continue their important work of providing meaningful AT access. However, gaining access to AT is only one of many steps towards PwADRD’s self-care and improved quality of life. With the fast advent of technology, individuals and society continue to evolve rapidly. Systematic changes are needed, not only in funding but also in infrastructure and human resource building, to support the adoption of the IoT ecosystem outlined in this chapter. Along with AT, these system changes will empower and engage PwADRD and their caregivers in its design, funding, use, and evaluation and, ultimately, enable PwADRD to lead meaningful lives.
6. Conclusions
In this chapter, we presented an assistive technology ecosystem that enables independence and promotes interdependence for PwADRD and their living environment. More than technology alone will be needed to solve the challenges PwADRD, their caregivers and our society face. Systematic changes, including user-centeredness in technology solutions, employment of participatory action methodologies for technology design and implementation, funding and care models are needed to create an affordable and sustainable ecosystem as outlined in this chapter.
Acknowledgments
The authors thank Drs. Susan Horton, Manoj Sachdev, Mahesh Tripunitara, John Long, Plinio Morita, Jennifer Boger, and Guang Gong for their contribution to the origination of the research proposal. This research is funded by the Centre of Biomedical and Biotechnology’s Seed Fund, awarded to Helen Chen and Mahesh Tripunitara.
Appendices and Nomenclature
Alzheimer’s disease and related dementia A person living with Alzheimer’s disease and related dementia Active Assisted Living Assistive Technology Internet of Things
References
- 1.
World Health Organization. Dementia [Internet]. 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/dementia. [Accessed: December 21, 2022] - 2.
Alzheimer Society of Canada. Dementia numbers in Canada [Internet]. 2022. Available from: https://alzheimer.ca/en/about-dementia/what-dementia/dementia-numbers-canada#ref1. [Accessed: December 21, 2022] - 3.
Alzheimer's Association. Alzheimer’s disease facts and figures. Alzheimer’s & Dementia. 2019; 15 :321-496 - 4.
Alzheimer's Society of Canada. Prevalence and Monetary Costs of Dementia in Canada. Alzheimer Society of Canada; 2016 - 5.
Columbus, L.. A roundup of 2018 enterprise Internet of things forecasts and market estimates. Comfort Life. Memory Care Costs. 2018. Available from: https://www.comfortlife.ca/retirement-community-resources/retirement-costs-ontario#memory-care - 6.
Public Health Agency of Canada. What we Heard Report: Informing a Dementia Strategy for Canada. Ottawa, Canada: Public Health Agency of Canada; 2019 - 7.
Dupuis SL, Epp T, Smale BJA. Caregivers of Persons with Dementia: Roles, Experiences, Supports, and Coping. Literature Review Prepared for the Ministry of Health and Long-Term Care and Ontario's Senior's Secretariat as Part of Ontario's Alzheimer Strategy (Imitative #6 – Research on Caregiver Needs). Waterloo, ON: Murray Alzheimer Research and Education Program; 2004. p. 111 - 8.
Fadrique FL, Rahman D, Morita PP. The active assisted living landscape in Canada. CSA Group. 2019. Available from: https://www.csagroup.org/article/the-active-assisted-living-landscape-in-canada/ ;https://preprints.jmir.org/preprint/15923 - 9.
Baum F, MacDougall C, Smith D. Participatory action research. Journal of Epidemiology and Community Health. 2006; 60 (10):854-857. DOI: 10.1136/jech.2004.028662 - 10.
Dupuis S, McAiney C, Loiselle L, Hounam B, Mann J, Wiersma EC. Use of participatory action research approach to develop a self-management resource for persons living with dementia. Dementia (London). 2021; 20 (7):2393-2411. DOI: 10.1177/1471301221997281 - 11.
Tiersen F, Batey P, Harrison MJC, Naar L, Serban AI, Daniels SJC, et al. Smart home sensing and monitoring in households with dementia: User-centered design approach. JMIR Aging. 2021; 4 (3):e27047 - 12.
Goeman DP, Corlis M, Swaffer K, Jenner V, Thompson JF, Renehan E, et al. Partnering with people with dementia and their care partners, aged care service experts, policymakers, and academics: A co-design process. Australasian Journal on Ageing. 2019; 38 (52):53-58. DOI: 10.1111/ajag.12635 - 13.
Mayer JM, Zach J. Lessons learned from participatory design with and for people with dementia. In: Proceedings of the 15th International Conference on Human-Computer Interaction with Mobile Devices and Services. New York: ACM Digital Library; 2013. pp. 540-545. DOI: 10.1145/2493190.2494436 - 14.
Bricout J, Greer J, Fields N, Xu L, Tamplain P, Doelling K, et al. The "humane in the loop": Inclusive research design and policy approaches to foster capacity building assistive technologies in the COVID-19 era. Assistive Technology. 2021; 34 (6):644-652. DOI: 10.1080/10400435.2021.1930282 - 15.
Herring J. Health as vulnerability; interdependence and relationality. The New Bioethics. 2016; 22 (1):18-32. DOI: 10.1080/20502877.2016.1151255 - 16.
Liu L, Daum C, Miguel Cruz A, Neubauer N, Perez H, Ríos RA. Ageing, technology, and health: Advancing the concepts of autonomy and independence. Healthcare Management Forum. 2022; 35 (5):296-300. DOI: 10.1177/08404704221110734 - 17.
Bennett CL, Brady E, Branham SM. Interdependence as a frame for assistive technology research and design. In: Proceedings of the 20th International ACM SIGACCESS Conference on Computers and Accessibility, ACM. New York, NY, USA: ASSETS '18; 2018. pp. 161-173. DOI: 10.1145/3234695.3236348 - 18.
Hoel V, Ambugo EA, Wolf-Ostermann K. Sustaining our relationship: Dyadic interactions supported by Technology for People with dementia and their informal caregivers. International Journal of Environmental Research and Public Health. 2022; 19 (17):10956. DOI: 10.3390/ijerph191710956 - 19.
Liu L, Daum C, Neubauer N, Cruz AM, Rincón AR. What is Autonomy and Independence in the Context of Aging in an Era of Technology?. In: Autonomy and Independence. Synthesis Lectures on Technology and Health. Cham: Springer; 2022. DOI: 10.1007/978-3-031-03764-1_1 - 20.
Lindemann K. The ethics of receiving. Theoretical Medicine and Bioethics. 2003; 24 :501-509 - 21.
Sobel K, Rector K, Evans S, Kientz JA. Incloodle: Evaluating an interactive application for young children with mixed abilities. In: Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems (CHI '16). New York, NY, USA: Association for Computing Machinery; 2016. pp. 165-176. DOI: 10.1145/2858036.2858114 - 22.
By Us For Us. Tips and Strategies. 2018. Available from: https://the-ria.ca/wp-content/uploads/2018/11/BUFU-Guide-Tips-and-Strategies_AODA.pdf - 23.
Danesh M, Long JR. An autonomous wireless sensor node incorporating a solar cell antenna for energy harvesting. IEEE Transactions on Microwave Theory and Techniques. 2011; 59 (12):3546-3555 - 24.
Saputra N, Long JR. A fully integrated wideband FM transceiver for low data rate autonomous systems. IEEE Journal of Solid-State Circuits. 2015; 50 (5):1165-1175 - 25.
Nabavi M, Sachdev M. A 290-mV, 3.34-MHz, 6T SRAM with pMOS access transistors and boosted wordline in 65-nm CMOS technology. IEEE Journal of Solid-State Circuits. 2017; 53 (2):656-667 - 26.
Patel D, Sachdev M. 0.23-V sample-boost-latch-based offset tolerant sense amplifier. IEEE Solid-State Circuits Letters. 2018; 1 (1):6-9 - 27.
Halperin D, Heydt-Benjamin TS, Fu K, Kohno T, Maisel WH. Security and privacy for implantable medical devices. IEEE Pervasive Computing. 2008; 7 (1):30-39. DOI: 10.1109/MPRV.2008.16 - 28.
AlTawy R, Rohit R, He M, Mandal K, Yang G, Gong G. sLiSCP: Simeck-Based Permutations for Lightweight Sponge Cryptographic Primitives. In: Adams C, Camenisch J, editors. Selected Areas in Cryptography – SAC 2017. Lecture Notes in Computer Science. Vol 10719. Cham: Springer; 2017. DOI: 10.1007/978-3-319-72565-9_7 - 29.
Dwork C, McSherry F, Nissim K, Smith A. Calibrating Noise to Sensitivity in Private Data Analysis. In: Halevi S, Rabin T, editors. Theory of Cryptography. Lecture Notes in Computer Science. Vol 3876. Berlin, Heidelberg: Springer; 2006. DOI: 10.1007/11681878_14 - 30.
Dewing J. From ritual to relationship: A person-centred approach to consent in qualitative research with older people who have a dementia. Dementia. 2002; 1 (2):157-171 - 31.
Dewing J. Participatory research: A method for process consent with persons who have dementia. Dementia. 2007; 6 (1):11-25 - 32.
Boger J, Mulvenna M, Moorhead A, Krul J, Bond R, Jutai J. Ethical issues in technology for dementia. In: Astell A, Smith S, Joddrell P, editors. Using Technology in Dementia Care: A Guide to Technology Solutions for Everyday Living. London and Philadelphia: Jessica Kingsley Publishers; 2019 - 33.
Boger J, Jackson P, Mulvenna M, Sixsmith J, Sixsmith A, Mihailidis A, et al. Principles for fostering the transdisciplinary development of assistive technologies. Disability and Rehabilitation: Assistive Technology. 2017; 12 (5):480-490. DOI: 10.3109/17483107.2016.1151953 - 34.
Hussein T, Boger J, Rudzicz F. The impact of design on feelings of trust of online information for family caregivers of people with dementia. In: Proceedings of the 32nd International BCS Human Computer Interaction Conference. Belfast United Kingdom, July 2018. Vol. 32. 2018. pp. 1-6 - 35.
Layton N, Steel E. The convergence and mainstreaming of integrated home Technologies for People with disability. Societies. 2019; 9 (4):69-80. DOI: 10.3390/soc9040069 - 36.
Hamblin K. Sustainable social care: The potential of mainstream "smart" technologies. Sustainability. 2022; 14 (5):2754. DOI: 10.3390/su14052754 - 37.
Marchand D, Nakhuda H, Dolcine B, Li Y, MacDougall D. Funding and access to assistive technologies: Electronic aids to daily living. Canadian Journal of Health Technologies. 2021; 1 (5). DOI: 10.51731/cjht.2021.68