
Abstract
Dengue is a viral disease caused by a flavivirus transmitted by Aedes aegypti mosquitoes in tropical regions but has spread to regions of Europe, subtropical regions, and South America. The clinic is varied, so imaging methods are important before having a positive confirmatory test. Clinically, dengue is a disease that increases vascular permeability with loss of plasma and albumin, causing polyserotis. The most accessible imaging methods in the emergency room are chest radiography and abdominal ultrasound. Chest radiography shows that the most frequent finding is pleural effusion. Abdominal ultrasound has several findings, including thickened gallbladder wall, ascites, and hepatic and splenomegaly. The thickened gallbladder wall is an indicator of disease severity since the more severe the thickening, the more severe the clinical picture. The patient’s platelet count is also related to the ultrasound findings, since the lower the platelet count, the more severe is the thickened gallbladder wall. The differential diagnosis of dengue should include other febrile states such as influenza, Zika, Chikungunya, and COVID-19.
Keywords
- dengue
- abdominal ultrasound
- pleural effusion
- gallbladder wall thickening
- ascites
1. Introduction
Dengue is the most important arboviral infection affecting humans and presents a major challenge for public health services worldwide.
Most infections are asymptomatic or result in only a brief systemic viral illness; a small proportion of patients develop potentially fatal complications.
Although dengue fever disease is mild in most cases and does not progress to severe disease, it can cause many cases in an epidemic form, resulting in overcrowding of health services. Therefore, the ability to recognize cases that progress to severe disease is important.
The World Health Organization classifies dengue into two main categories: dengue with or without warning signs and severe dengue. The secondary classification of dengue with or without warning signs is designed to assist health care professionals in selecting patients for hospital admission for close observation and to minimize the risk of progression to the more severe form of dengue.
The differential diagnosis should be made with febrile states (especially if it is in time of dengue epidemic), such as influenza, Zika, Chikungunya, Hanta Virus (in regions with endemic cases of hanta), and COVID-19.
2. Imaging methods
The most frequently used imaging methods in dengue are chest radiography and abdominal ultrasound, especially in emergency rooms.
The initial evaluation of a patient with dengue is with chest X-ray, and according to the clinical picture and its evolution, other diagnostic methods are requested [1, 2].
Dengue consists of a significant increase in vascular permeability, with loss of plasma and albumin from the intravascular space, causing polyserositis.
Abdominal ultrasound is a widely available imaging technique to study abdominal pain and acute febrile processes. It allows to assess with a high degree of certainty the abdominal findings related to dengue fever, which are thickening of the gallbladder wall, ascites, hepatomegaly and splenomegaly, pericardial effusion, and pleural effusion [2, 3, 4].
In chest radiography, pleural effusion is the most frequent finding, which can be unilateral or bilateral, of variable quantity and mainly on the right side. In cases of severe dengue, it may demonstrate the presence of vascular congestion or lead to acute respiratory distress syndrome [4, 5].
3. Imaging findings related to dengue fever
3.1 Gallbladder wall thickening
It is one of the most frequent findings, but it is non-specific since it is found in other viral infections, cholecystitis, liver cirrhosis, and portal hypertension. There are different forms of gallbladder wall thickening that can be observed in ultrasound. These can be lamellar or layered, diffuse, and reticular thickening. Of these forms of thickening, the diffuse thickening is the most frequent form. Lamellar and reticular thickening are observed more frequently in children or young adults. Reticular thickening is more frequent in patients with severe dengue. This type of thickening is usually located at the bottom of the gallbladder Figures 1 and 2 [4, 5].
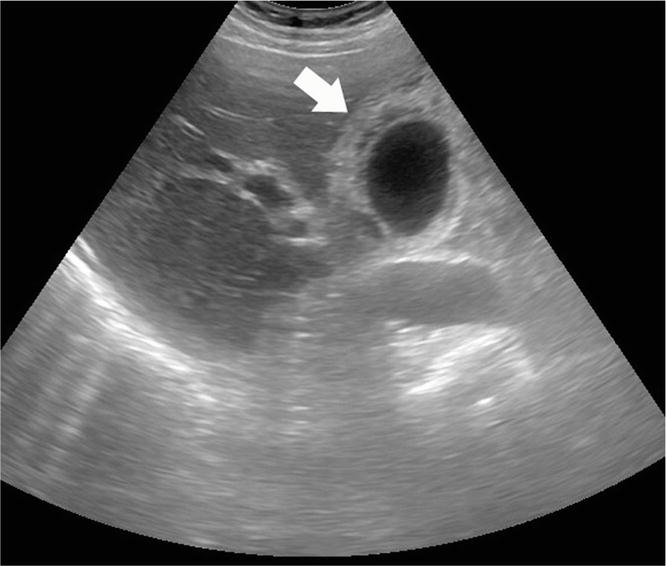
Figure 1.
Abdominal ultrasound axial section. Diffuse gallbladder wall thickening is observed diffusely, (white arrow).
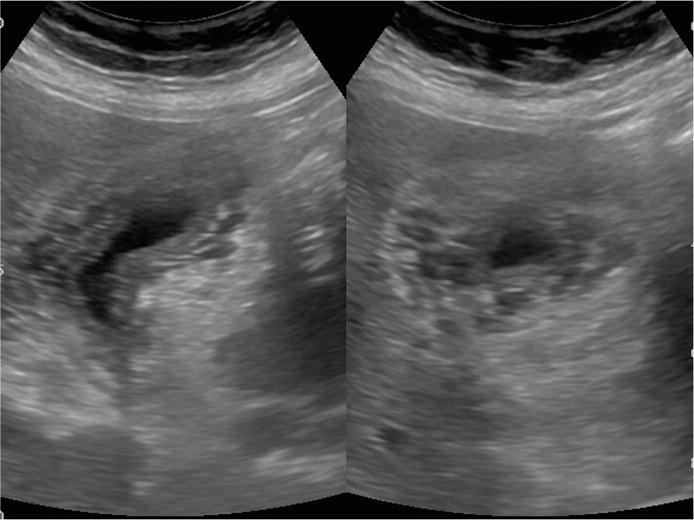
Figure 2.
Abdominal ultrasound. Gallbladder wall thickening with ill-defined lamellar appearance.
3.2 Ascites
Ascites develops with the pathophysiological process of polyserositis, correlating with the severity of the disease. Ascites is detected on physical examination when it exceeds 1000 cc in volume, while ultrasound can demonstrate the existence of scant amounts of peritoneal fluid (approx. 100 cc). Its appearance is usually anechoic and may be of variable quantity. Figures 3 and 4 [5, 6].
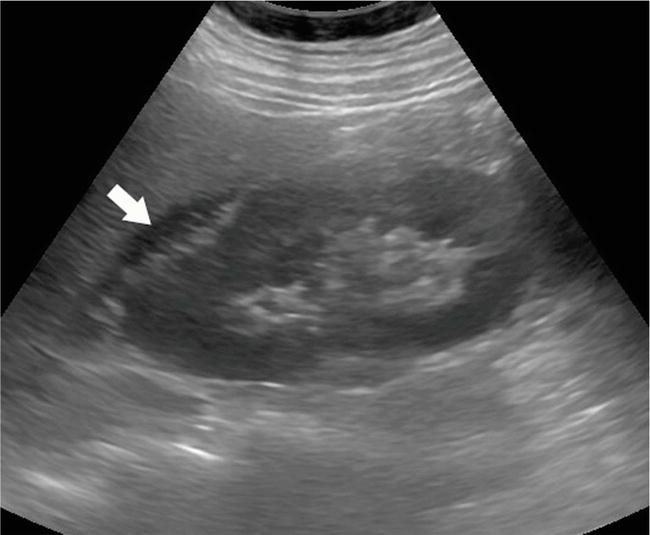
Figure 3.
Abdominal ultrasound. The presence of free fluid around the right kidney is observed at the level of Morrison’s fossa (White arrow).
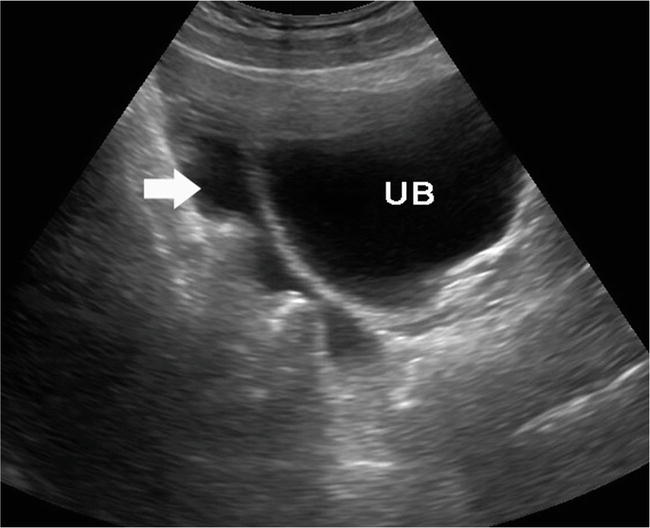
Figure 4.
Free fluid in the pelvic excavation. UB: urinary bladder, (White arrow).
3.3 Pleural effusion
As in ascites, pleural effusion is part of the process of polyserositis, resulting in plasma leakage into the pleural cavity. It is generally an infrequent finding being right or bilateral. Pleural effusion in dengue is one of the markers of severity, but it is mild and self-limiting without the need for intervention. The type of pleural effusion is exudative. Figures 5 and 6 [4, 5, 6, 7].
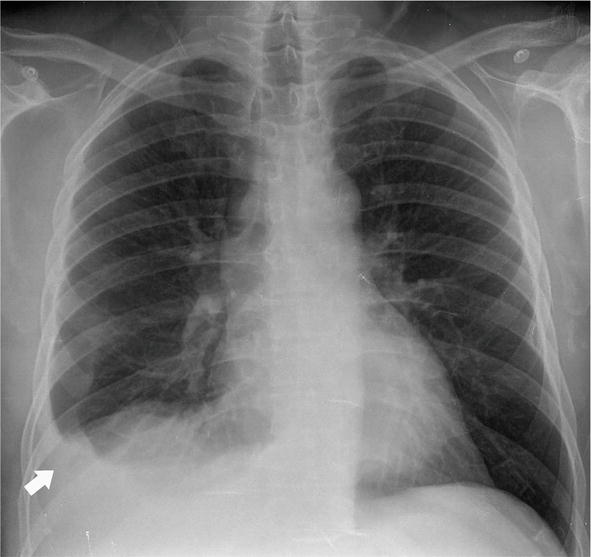
Figure 5.
Chest X-ray. Right costal diaphragmatic angle obliteration due to pleural effusion (arrow).

Figure 6.
Abdominal Ultrasound. Transverse hepatic view. Shows simple pleural effusion on the right side (White arrow).
3.4 Hepatomegaly and splenomegaly
Both hepatomegaly and splenomegaly’s growth is homogeneous, without focal lesions. In some cases, the liver may present steatosis. Liver growth may be present in up to 30% of cases of dengue fever. Splenomegaly may be present in 14% of cases. Figure 7 [7].
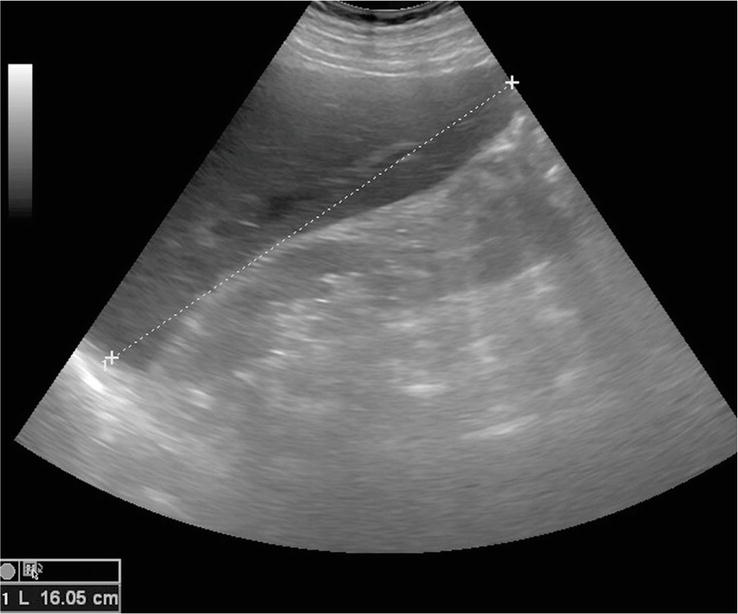
Figure 7.
Abdominal Ultrasound. Hepatic cross-sectional view. Shows mild liver enlargement with homogeneous liver parenchyma.
3.5 Pericardial effusion
It may occur in severe cases after the fifth or seventh day of illness in up to 28% of cases. Its sonographic characteristic is a simple anechoic effusion [7, 8].
There may be a combination of sonographic findings in a patient with a diagnosis of dengue. We can find gallbladder wall thickening with ascites and pleural effusion at any age.
4. Platelet count and imaging findings
Several hematological parameters have been considered as potential predictors, most commonly the platelet count.
The severity of the course of the disease, which is directly linked to the platelet count, can also be assessed by sonography.
In patients whose platelet counts are less than 40,000, the most frequent findings are gallbladder wall thickening, ascites, and pleural effusion. With platelet counts between 40,000 and 80,000, the most frequent findings are gallbladder wall thickening and pleural effusion. With platelet counts greater than 80,000, pleural effusion is more frequent followed by gallbladder wall thickening [7].
5. Conclusion
In the clinical context of a patient with suspected dengue fever, findings of gallbladder wall thickening, ascites, pleural effusion, and hepato-splenomegaly strongly favor the diagnosis of dengue fever. An abdominal ultrasound examination can effectively recognize these and guide the clinician to initiate prompt treatment without waiting for serologic results. Ultrasound can also estimate the severity of the disease. The degree of thrombocytopenia shows a direct relationship with abnormal ultrasound findings.
References
- 1.
Castrillón ME, Iturrieta N, Cativelli S, Padilla F. Hallazgos ultrasonográficos en pacientes con Dengue. Revisión de la literatura. Revista argentina de radiología. 2010; 75 :71-76 - 2.
Sophie Y, Bridget W. Predicting outcome from dengue. BMC Medicine. 2014; 12 :147 - 3.
Basawaraj NG, Dasan TA, Patil SS, Deepashri B. Sonography in the diagnosis and assessment of dengue fever. International Journal of Research in Medical Sciences. 2015; 3 (11):3131-3136 - 4.
Venkata Sai PM, Krishnan R. Role of ultrasound in dengue fever. British Journal of Radiology. 2005; 78 :416-418 - 5.
Sachar S, Goyal S, Sachar S. Role of ultrasonography (“Honeycomb Sign”) in early detection of dengue hemorrhagic fever. Archives of Clinical and Experimental Surgery. 2013; 2 (1):38-42 - 6.
Oliveira GA, Machado RC, Horvat JV, et al. Transient reticular gallbladder wall thickening in severe dengue fever: A reliable sign of plasma leakage. Pediatric Radiology. 2010; 40 :720-724 - 7.
Vedaraju KS, Vijay Kumar KR, Vijayaraghavachari TV. Role of ultrasound in the assessment of dengue fever. International Journal of Scientific Study. 2016; 3 :59-62 - 8.
Shabbir M, Ameen F, Roshan N, Israr M. Nature and clinical course of pleural effusion in dengue fever. Internal and Emergency Medicine. 2018; 1 (1):1006