
Abstract
The current literature covers the role of selenium in metabolic processes and the importance of correcting its level in various diseases and critical conditions, including acute cerebral damage due to severe traumatic brain injury (TBI) and sepsis-associated encephalopathy (SAE). Numerous experimental animal studies have demonstrated that selenium has protective properties and blocks the mechanisms of apoptosis, and is involved in maintaining the functional activity of neurons and inhibits astrogliosis. The study of the selenium content in the blood of patients with acute cerebral damage due to severe TBI and sepsis with verified SAE, and the development of schemes of replacement selenium therapy will improve outcomes, both in increasing survival and in reducing the resuscitation bed-day and the number of neurological deficits in the future.
Keywords
- replacement selenium therapy
- acute cerebral damage
- severe traumatic brain injury
- sepsis-associated encephalopathy
1. Introduction
Selenium is an essential trace element in the human body. Normally, the concentration of selenium in blood plasma is 100–200 mcg/l. The most studied function of selenium is the regulation of antioxidant processes in all organs and tissues, primarily in the central nervous system [1]. Selenium deficiency leads to an imbalance of the lipid peroxidation/antioxidant system, which is a constant component of any pathological process [2, 3]. Selenium deficiency provokes structural changes in the membranes of microsomes, and damage to the organoid membranes of cells of almost all tissues and it is accompanied by a change in the activity of 5-nucleotidase, creatine phosphokinase, LDH, b- hydroxybutyrate, AST, ALT, aldolase, Na, and K-ATPase [4, 5].
Experimental animal studies have demonstrated that selenium has protective properties and blocks the mechanisms of apoptosis-cell death, and participates in maintaining the functional activity of neurons and in inhibiting astrogliosis in the acute cerebral injury of various etiologies [6, 7, 8, 9, 10].
It is known that selenium-dependent proteins—the family of glutathione peroxidases (GPX1-6), as well as selenoproteins P, W, T, M, etc. play a key role in the processes of inhibition of free radical oxidation chain reactions [4, 5].
The function of glutathione peroxidases is to maintain stable intracellular concentrations of reduced glutathione. Cytosolic glutathione peroxidase (GPX1) plays a major protective role in the development of oxidative stress. GPX1 activity is more dependent on selenium content compared to other enzymes, and therefore GPX1 activity in erythrocytes is a simple and sensitive indicator of the selenium status of the organism [11]. Intracellular and tissue levels of GPX1 also affect the activity of apoptotic pathways and phosphorylation of protein kinases [12].
Selenoprotein P, being the main extracellular source of selenium, performs the function of selenium transport to various tissues, mainly to the brain [13, 14], as well as antioxidant functions [15, 16], normally amounts to 6–7 micrograms of selenium/dl plasma.
Thus, selenium is a very important micronutrient for adequate function of the brain. The role of selenium is to protect against oxidative stress and other damaging factors in the central nervous system [17], maintaining the balance of neurotransmission and inflammation control [18].
2. Selenium metabolism in critical conditions
The study of the dynamics of antioxidant systems and lipoperoxidation processes made it possible to clarify the basic pathophysiological mechanisms underlying the development of critical conditions [19, 20, 21]. Activation of the processes of lipid peroxidation and oxidative modification of plasma proteins, which leads to a violation of the structural and functional integrity of membranes, inactivation of protein enzymes, and impaired synthesis of nucleic acids and protein, is a universal damaging mechanism in severe trauma and critical conditions of any genesis [22, 23]. Ischemic-reperfusion injury often accompanies severe forms of systemic inflammatory reactions, exacerbating the harmful effects of free radicals, and leading to an imbalance between oxidation processes and antioxidants. This situation has already been described in patients with sepsis and non-septic forms of systemic inflammatory syndromes in which there is a significant increase in the production of free radicals, especially superoxide anions [24].
In critical conditions, there is an increasing consumption of selenium and insufficient intake of it into the body from the outside, which leads to a deficiency of selenium in the body and makes it defenseless when exposed to oxygen free radicals and the cascade of reactions caused by their activation [25, 26, 27].
Selenium exhibits significant antioxidant activity, preventing changes in cell membranes, participates in respiratory chain reactions, in the pentose phosphate cycle, in the citric acid cycle, and lipid peroxidation [28]. Selenium activates protein synthesis, participates in antihistamine and antiallergic mechanisms, and normalizes the metabolism of proteins and nucleic acids [29].
Pathogenetic substantiation for the use of selenium in the intensive care complex in critical conditions, according to a number of authors [30, 31, 32, 33, 34], consists in the following mechanisms of action:
Suppression of endothelial adhesion and protection of the endothelium from damage by oxygen radicals;
Reduced production of pro-inflammatory cytokines;
Suppression of hyperactivity of the nuclear factor NF-kB;
Decrease in the activity of the complement system;
Maintaining the utilization of peroxides;
Stabilization of glucocorticoid receptors;
Stimulation of the insulin signaling cascade due to an insulin-like effect that improves glucose control.
The above mechanisms of action contribute to the prevention of microcirculatory-mitochondrial dysfunction as a universal link of multiple organ failure [35, 36, 37].
Selenium plays an important role in the functioning of the immune system. Thus, in conditions of selenium deficiency, the processes of antigen-dependent lymphocyte proliferation, neutrophil chemotaxis are disrupted, and the level of IgA, IgG, and IgM decreases [24, 29].
A relationship was established between the low concentration of selenium in the blood serum and the severity of the condition of patients, and the level of mortality, which served as the basis for the early inclusion of selenium in the intensive care regimen for critical conditions [38, 39, 40]. The introduction of sodium pentahydrate selenite ensures normalization of plasma selenium concentration in the next 24 hours, leads to improved functioning immunocompetent cells (increased phagocyte activity, T-killer activity, immunoglobulin synthesis, etc.), contributes to improving clinical outcomes and significantly reducing patient mortality [41, 42]. Appointment of sodium selenite in patients in critical condition with infectious systemic inflammatory response ensures normalization of plasma selenium concentration in the next 24 hours. Numerous studies have shown that among patients in critical condition and suffering from sepsis, among those who underwent correction of selenium deficiency, mortality was significantly lower than in patients who did not receive selenium preparations [43, 44, 45, 46, 47, 48, 49, 50, 51]. The combination of selenoprotein P for endothelial protection and the cytotoxic effects of Na2SeO3 against hyperactivated leukocytes may be a promising intervention for early sepsis [52]. Copper-selenium nanoclusters may be an efficient strategy to cure sepsis by
According to the experts of the Cochrane Collaboration [22], concerning studies on selenium exchange in critically ill patients based on an analysis of seven randomized clinical trials, the quality of the studies was not good enough, the availability of outcome data was often limited, and studies examining the effects of selenium replacement therapy were insufficient in size of the study population. In addition, the main problem of these studies was related to the heterogeneity of the studied patient population, as a result of which the results are presented in the form of random effects. Most of the analyzed papers were statistically insignificant. Based on all of the above, the Cochrane Collaboration experts concluded that there is insufficient evidence of the effectiveness of selenium therapy at the present time in relation to the duration of ventilation, bed-day in intensive care, general hospital bed-day or quality of life after a critical condition, to recommend it for use in patients in critical condition. Meanwhile, some authors believe that the inclusion of selenium-containing drugs in the intensive care complex opens up new horizons in the treatment of critical conditions [54]. Note also that in a systematic review by Berger et al. [28], Shenkin [55] provides data on the feasibility of short courses of intravenous use of selenium in patients in critical condition (burns, serious injuries, sepsis, and stroke).
Since 2009, selenium has been included in the ESPEN recommendations as a pharmacological module (Grade C) [56], since 2010—in the national guidelines for the treatment of sepsis in Germany (Grade C) [57, 58].
Among the patients in critical condition, patients with sepsis and polytrauma, including TBI, require the most attention. The role of selenium in the regulation of inflammatory response and gene transcription mechanisms in patients with polytrauma is discussed by a number of authors [59]. Most patients who are in a prolonged unconscious state suffer sepsis at different periods of their disease against the background of low plasma selenium levels [60]. At the same time, the constant administration of various groups of antibacterial drugs often does not affect the frequency of septic complications development and leads only to the formation of polyresistant flora.
In one study carried out by Chelkeba et al. [61], the antioxidant effect of selenium was researched in 54 patients under critical condition due to severe sepsis and septic shock, or mechanically ventilated for more than 48 hours [61]. Twenty-nine patients (1st group) received 2000 μg of sodium selenite in 100 ml of saline solution within the first 6 hours of sepsis diagnosis, followed by 1500 μg of sodium selenite in 250 ml of saline solution for 12 hours continuously for 14 days, had mortality rates lower (31%) then 25 patients (2nd group) with intensive standard treatment without selenium (40%). Also, it was found a significant increase in GPx-3 levels, which causes a blocking action of the inflammatory cytokines [61].
Another clinical study by G. Landesberg with colleagues [62] showed a negative correlation between pro-inflammatory cytokines and the severity of sepsis and myocardial dysfunction assuming that selenium has no effect in septic patients since this nutrient did not present any long-term effect on the pro-inflammatory cytokines plasma concentration [62].
Kieliszek and Lipinski [63] demonstrated that sodium selenite can oxidize thiol groups in disulfide isomerase proteins of the SARS CoV-2 virus, thus preventing the COVID-19 virus from penetrating the membrane of healthy cells of its possible hosts. Such hypotheses can be considered about selenium since this nutrient is of great importance for inflammatory diseases [63].
The study by Mahmoodpoor et al. [64] did not indicate the presence of adverse events related to the high dose of intravenous sodium selenite and aspects of toxicity from its administration [64].
In one meta-analysis selenium supplementation for severe trauma patients was examined. The current evidence supports that selenium administration decreases the mortality rate and ICU and hospital stays for patients who have sustained major trauma. Selenium supplementation was not associated with infectious complications after major trauma [65]. Selenium administration shows no substantial influence on the 28-day mortality, length of ICU stay, duration of vasopressor therapy, incidence of acute renal failure, and serious adverse events for septic patients [66].
Some multiple-center trials confirm the efficacy of high-dose sodium selenite supplementation in patients with severe sepsis and septic shock to reduce 28-day mortality [67].
However, in Valenta et al. [68] study, it was shown that the 28-day mortality is not decreased after selenium administration in septic patients and in critically ill patients [68].
3. Selenium homeostasis in the brain
Insufficient selenium supply and lack of selenoprotein function have been linked to multiple brain disorders, including neurodegenerative diseases, which have been thoroughly discussed in previous reviews [8, 10]. Conversely, selenium has been suggested as a potential therapeutic agent in the treatment of Alzheimer’s disease [11], multiple sclerosis [12], and stroke [13, 69, 70, 71, 72].
Great importance is attached to the provision of the body with selenium in the occurrence of neurodegenerative diseases (Alzheimer’s disease, Parkinson’s disease) [69, 73]. The largest and most well-organized study [74], conducted in 2003–2005 in two provinces of China and included 2000 people, showed that low selenium content in nails directly correlates with a decrease in intelligence in people over 65 years of age (p < 0.0087). In this regard, selenium preparations are considered promising in the prevention and treatment of Alzheimer’s type dementia. In addition, Thiel and Fowkes [75] showed that the use of an antioxidant complex prevents the development of dementia in children with Down’s disease (this population represents the largest cohort with an increased risk of dementia due to overexpression of the superoxide dismutase gene) [75].
Another important potential use of selenium is for Parkinson’s disease [76]. It is proved that there is a significant increase in the disease prooxidant processes, and the activity of glutathione reductase and other antioxidant enzymes increases compensatorily [77]. At the same time, a study by Kim et al. [78, 79] showed that the use of selenium significantly weakened the phenomena of oxidative stress caused by methamphetamine in nigrostriatal neurons, thus preventing the development of experimental parkinsonism [78, 79]. Note, however, that the concentration of selenium in the cerebrospinal fluid is increased in all patients with Parkinson’s disease.
Perhaps this reflects the increased utilization of selenium under conditions of severe oxidative stress in these patients [80]. Recent studies suggest a significant role of selenium and the enzyme glutathione peroxidase in the pathogenesis of epilepsy [81, 82]. Decreased activity of Se-BP1 (selenium-binding protein 1) pathognomonic for schizophrenia, with exacerbation it decreases to critical figures, and with replenishment, there is an improvement in the condition [83].
An important role is played by the change in the antioxidant status in ischemic stroke. In the study of Zimmermann et al. [84], it was shown that on the first day after a stroke, a significant decrease in selenium levels (p < 0.01) was observed against the background of increased glutathione peroxidase activity (p < 0.01) [84]. Numerous experimental studies [85, 86] demonstrated distinct neuroprotective properties of selenium in conditions of cerebral ischemia. Ansari et al. [85] demonstrated the neuroprotective effect of different doses of selenium (from 0.05 to 0.2 mg/kg) on models of occlusion of the middle cerebral artery [85]. A study by Yousuf et al. [87] showed that the use of selenium in the form of sodium selenite (0.1 mg/kg) led to a significant recovery of ATP levels in the neurons of rats subjected to cerebral ischemia (p < 0.05–0.001) [87]. In addition, there was a decrease in the area of edema and microglia infiltration.
Wray J. R. et al. [88] and Perez A. with colleagues [89] demonstrated the glucocorticoids influence on the selenoproteins regulation [88] and the metabolic effects of glucocorticoids, which include over-eating and excess weight gain [89].
The neuroprotective effect of selenium as a result of selenium replacement therapy in patients with neurological deficiency after subarachnoid hemorrhage of aneurismal etiology was noted by Japanese colleagues [90]. Japanese authors also described the positive effect of the inclusion of ebselen in the complex therapy of ischemic stroke [91]. It should be noted that the selenium-containing drug ebselen is currently undergoing the registration procedure for applications for stroke and subarachnoid hemorrhage in Japan.
The proposed scheme of the main physiological processes involved in the specific mechanisms of selenium uptake by the brain is shown in Figure 1 [92].
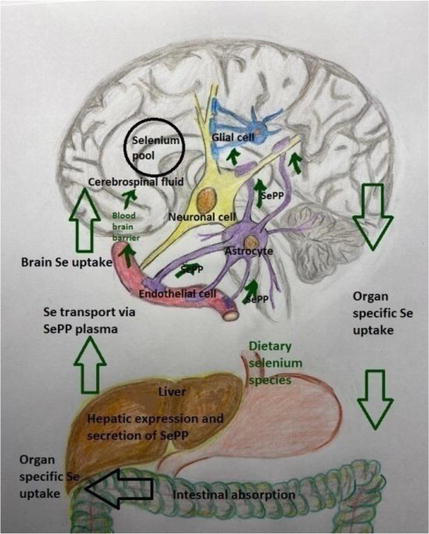
Figure 1.
Scheme of the main physiological processes involved in the mechanism of specific selenium uptake by the brain [
In the experimental study by Xu L. with colleagues [93] was shown that plasma selenium levels were lower in the Chronic Unpredictable Mild Stress (CUMS)-sensitive group of rats [93]. It is important that an epidemiological study correlated low selenium intake with an increased susceptibility for developing the major depressive disorder in humans [94].
4. The role of selenium in preventing apoptosis and cerebral damage (according to the results of experimental studies)
In the experimental works of R.F. Burk et al. [95, 96], it was shown that the introduction of sodium selenite leads to a significant increase in the content of selenoprotein P in the brain (compared with other tissues), and in conditions of selenium deficiency, the brain’s uptake of selenoprotein P increases by five times; at the same time, low-molecular selenium compounds are not utilized by the brain [95, 96]. Moreover, the research of P. R. Hoffmann et al. [97] showed that genetic deficiency of selenoprotein P in transgenic mice leads to a decrease in the expression of other selenoproteins in the brain; presumably, this is due to the mechanism of selenoprotein biosynthesis: in conditions of cellular selenium deficiency, the UGA codon encoding selenocysteine begins to play the role of a stop codon, and the synthesis of selenium protein is interrupted [97].
In experiments on rats in the early period of TBI (after 6 hours and 24 hours), there was a sharp decrease in the level of selenium and vitamin E in the blood of animals [7]. The reason for the decrease was oxidative stress and a high level of selenium consumption. Therefore, according to the authors of the study, it is necessary to restore selenium levels to normal values preceding TBI.
In an experimental model of cerebral ischemia/reperfusion in rats created by occlusion of the right carotid artery for 45 minutes, animals were treated with ginkgo biloba (50 mg/kg/day intraperitoneally) and selenium (0.625 mg/kg intraperitoneally) for 14 days after occlusion [98]. The activity of superoxide dismutase and glutathione peroxidase enzymes was measured in hippocampal tissue in 25 animals. An immunohistochemical study was performed with electron and light microscopy. According to the results of the study, the authors concluded that through the suppression of oxidative stress processes, a significant effect of neuroprotection in ischemia/reperfusion is realized with the combined use of ginkgo, selenium, and their combination [98]. Thus, data presented in the study by G. Erbil et al. [98], demonstrate that selenium treatment after ischemic/reperfusion injury improves the activity of antioxidant enzymes, prevents neuronal damage and moderate reactive gliosis caused by this kind of damage in the hippocampus in rats [98].
The inclusion of selenium as monotherapy or in combination with ginkgo significantly reduces brain tissue damage in this experimental model. Casaril A. M. with colleagues [99] showed that 3-((4-chlorophenyl)selanyl)-1-methyl-1H-indole (CMI) can prevent acute stress-induced depressive-like behavior in mice [99]. Also, CMI induces antinociceptive effects in mice by modulating serotonergic activity [100] and can reverse the depressive-like phenotype caused by lipopolysaccharide injection [101].
It is obvious that the results obtained
Oxidative stress, which is a universal pathophysiological mechanism in polytrauma, combined trauma and TBI, leads to the development of reactive gliosis in TBI. Damage to the astroglia may be a significant contribution to the formation of neuronal damage. It is well known that ischemia/reperfusion induces neuronal damage through several pathophysiological mechanisms, including intracellular Ca++ movement and free radical production, which ultimately triggers apoptosis. In the body, selenium protects cells from free radicals and peroxidase activity caused by oxidative damage, at the molecular level, selenium has neuroprotective properties in the brain [105, 106, 107, 108].
Several selenoproteins are expressed in the brain. Among them, according to the literature, the antioxidant effect of selenoprotein P on neuronal survival has been proven [109], and the role of neuronal selenoprotein is in the development of interneuronal connections and the prevention of seizures and the process of neurodegeneration [110]. However, its role in postischemic neuronal death cannot yet be explained.
With TBI, a reactive glial response is possible in the form of the development of astrogliosis-reactive gliosis in the hippocampus, and in the form of cellular hypertrophy, hyperplasia, increased release of glial fibrillar acid proteins.
The last study by O. Leiter et al. [111] has demonstrated that selenium mediates the exercise-induced increase in adult hippocampal neurogenesis, increases hippocampal precursor proliferation and adult neurogenesis, and reverses cognitive decline in aging and hippocampal injury [111].
Naziroglu et al. [9] did experimental work on rats, having created a hypoxic model of brain damage (convulsive seizures provoked by the administration of pentylenetetrazole). Selenium was preemptively injected at a dose of 0.3 mg intraperitoneally, then the activity of Ca++ -ATP-aza, the level of oxidative stress were measured for 7 days, and EEG was recorded in animals with affected brains [9]. The authors’ conclusion: selenium caused protective effects on pentylenetetrazole-induced brain damage due to reduced production of free radicals, regulation of Ca++ − dependent processes, and maintenance of the antioxidant system.
The literature also mentions information that selenium deficiency in chickens caused a decrease in the activity of glutathione peroxidase, the level of expression of the mRNA glutathione peroxidase gene, the development of oxidative stress of brain tissue, hypothyroidism, alterations in ion profiles in chicken muscles, imbalance in Ca ++ homeostasis, and then morphological damage to nervous tissue [112].
In an experimental model of TBI in mice, analysis of key regulators of apoptosis during H2O2-induced apoptosis in cells showed that selenium blocks the activation of certain protein kinases (JNK)/38, triggering apoptosis in neuronal cells [6].
Ozbal and colleagues [8] evaluated the levels of synthesis of tumor necrosis factor TNF-α and IL-1β, nerve tissue growth factor (NGF) in a cerebral ischemia/reperfusion model in rats [8]. In this study, they studied the effect of selenium on the prefrontal cortex and the degree of damage to the hippocampus in rats subjected to cerebral ischemia-reperfusion injury. Selenium was administered intraperitoneally to animals at a dose of 0.625 mg/kg/day after the onset of ischemic injury. Conclusion of the authors of the study: selenium treatment after ischemia significantly reduces the induced ischemia and subsequent reperfusion neuronal death in the prefrontal cortex and hippocampal CA 1 region in rats.
Selenium treatment reduces the levels of markers of systemic inflammatory response and tissue damage (TNF-α and IL-1β) and leads to an increase in the values of nerve tissue growth factor (NGF). B. Yang et al. [113] study was to explore the molecular mechanisms underlying the protective effects of selenium on the blood-brain barrier (BBB) following ischemia/reperfusion injury in hyperglycemic rats [113]. Treatment with selenium and the autophagy inhibitor 3-methyladenine significantly reduced cerebral infarct volume, brain water content, and Evans blue leakage, while increasing the expression of tight junction (TJ) proteins and decreasing that of autophagy-related proteins. It was revealed that selenium increased TJ protein levels, reduced BBB permeability, decreased autophagy levels, and enhanced the expression of phosphorylated (p)-AKT/AKT and p-mTOR/mTOR proteins [113].
In a study on mice, it was demonstrated that melatonin and selenium may serve as potential therapeutic targets against docetaxel-induced toxicity in the hippocampus and the brain (docetaxel is widely used to treat several types of glioblastoma) [114].
Summarizing the above, it can be argued that the results of experimental studies allow us to make the assumption that the introduction of selenium prevents the development of secondary pathological processes in the brain during its traumatic injury. Clinicians, based on the data of experimental works performed on animals, can propose new goals of drug therapy for the treatment of TBI from the bench to the bedside.
5. Replacement selenium therapy in severe traumatic brain injury
Positive clinical responses obtained during therapy with N-acetylcysteine and selenium in neurodegenerative diseases have provided substantial evidence for the important role of reactive oxygen species in pathological processes of TBI [6]. It is proved that the level of oxidative stress in severe TBI determines the severity of the processes of necrobiosis and neuronal death [5].
Works concerning selenium metabolism in patients with severe trauma, including traumatic brain injury, are isolated [11, 23, 115, 116, 117, 118, 119, 120].
In one study, a double-blinded controlled trial was carried out on 113 patients who were hospitalized following traumatic brain injury (TBI) with Glasgow Coma Scale score of 4–12 that were randomly assigned to receive selenium within 8 h after injury plus standard treatment group or routine standard treatment alone as the control. There was no difference in the length of ICU and hospital stay, the trend of the change in FOUR and SOFA scores within 15 days of first interventions, and the mean APACHE III score on the 1st and 15th days between the two groups. Mortality was 15.8% in the selenium group and 19.6% in the control group with no between-group difference. This human trial study could not demonstrate the beneficial effects of intravenous infusion of selenium in the improvement of outcomes in patients with acute TBI [120].
Several studies examine the effect of intravenous selenium (Selenase ®) treatment in patients with severe TBI on functional outcome and survival. Intravenous Selenase ® treatment demonstrates a significant improvement in functional neurologic outcomes [115]. H. S. Nutsalova in her study showed that selenium replacement therapy with Selenase ® at a dose of 1000 mcg/day for 12 days of the acute period of TBI significantly reduces the plasma level MDA (malonic aldehyde) in patients with severe TBI starting from day 7, reaching maximum intragroup and intergroup differences by day 12 (p < 0,01) [119]. Substitution selenium therapy does not affect the recovery time of consciousness in patients with severe TBI in the acute period of trauma. Replacement selenium therapy in patients with isolated and combined severe TBI provides the restoration of plasma levels of selenium and the sanogenetic orientation of free radical oxidation processes in the acute period of trauma. The known method of intravenous selenium use leads to a reduction in the duration of ventilation and a decrease in 28-day mortality in patients with severe TBI [116, 117, 118, 119].
6. Nontraumatic acute cerebral damage
Hirato J et al. [121] demonstrated in their observation that the brain lesions of the megacystis microcolon intestinal hypoperistalsis syndrome (MMIHS) patients mainly resulted from oxidative damage of the brain related to the low levels of glutathione peroxidase and other selenoproteins due to selenium deficiency [121]. The authors showed that long-term total parenteral nutrition is possibly due to selenium deficiency. Both patients described in the article died of sepsis. In both cases, severe neuronal loss and gliosis were present in the medial convolutions of the occipital lobe, including the visual cortex [121].
Perinatal hypoxic-ischemic encephalopathy (HIE) is an important cause of brain injury in the newborn and can result in devastating consequences. The principle mechanism underlying neurological damage in HIE, resulting from hypoxemia and/or ischemia is deprivation of glucose and oxygen supply which energy failure. A consequent reperfusion injury often deteriorates the brain metabolism by increasing oxidative stress damage. Selenium is a constituent of the antioxidant enzyme glutathione peroxidase and is vital to antioxidant defense.
Neonates with HIE had lower serum selenium level than normal healthy neonates, which is not dependent on the maternal serum selenium levels and was negatively correlated with the severity of HIE [122].
Neonatal mortality continues to be a significant problem in the Indian setting, especially in very low birthweight (VLBW) neonates. India is a selenium-deficient country. Blood selenium concentrations in newborns are lower than those of their mothers and lower still in preterm infants.
Preterm VLBW neonates are selenium deficient at birth. Selenium supplementation at 10 μg/day resulted in getting the selenium levels into the acceptable normal level and reduced the incidence of the first episode of late-onset sepsis in these neonates [123].
7. Sepsis-associated encephalopathy and selenium status: perspectives of replacement therapy
Septis-associated encephalopathy is an early manifestation of systemic infection when the focus of infection is outside the central nervous system (CNS), but the systemic inflammatory response causes organ dysfunction, including the brain. Researchers identify a number of factors and mechanisms that play a key role in the development of septis-associated encephalopathy: the effect of inflammatory mediators on the brain, inadequate cerebral perfusion pressure, impaired permeability of the blood-brain barrier (BBB), disorders of the cerebral microcirculation, cerebral ischemia, metabolic disorders, changes in amino acid levels, imbalance of mediators, liver failure, and multiple organ failure [124, 125]. BBB dysfunction largely explains the pathophysiology of SAE, since the central nervous system becomes highly sensitive to neurotoxic factors, such as free radicals, inflammatory mediators, intravascular proteins, plasma, and circulating leukocytes. Due to the barrier deficiency, brain edema is formed and microvascular perfusion decreases, which leads to the loss of neurons during SAE [125].
Microglial cells are the primary inducers of immune responses in the brain. Recent experimental studies have shown that microglial cells migrate to brain vessels during systemic inflammation and that their activation represents one of the earliest changes observed in SAE [126, 127].
Designed to protect against sepsis, microglia activation generates cytotoxic substances that release reactive oxygen species (ROS), nitric oxide (NO), and glutamate SAE [127]. Persistent microglial activation and excessive release of inflammatory mediators and free radicals trigger a vicious cycle of a circle leading to the aberrant function of neurons and cell death, contributing to the progression of SAE [128]. Data from some experimental studies indicate that glial activation plays a key role in the development of SAE and BBB dysfunction along with a deficiency of brain neurotrophic factors [128, 129].
The pathophysiology of SAE is a multifactorial process that involves a violation of the mechanism of cell death. Ferroptosis is a new form of programmed cell death characterized by the accumulation of iron and lipid peroxidation, which leads to an inflammatory cascade and the release of glutamate. Scientists have suggested that ferroptosis is involved in glutamate-mediated excitotoxic damage to neurons during an uncontrolled inflammatory process in SAE [130].
Assessment of neurological status and neurocognitive deficit and their dynamics are the criteria for the effectiveness of treatment of neurocognitive disorders in patients with sepsis-associated encephalopathy, along with clinical and laboratory indicators and scales for assessing multiple organ failure (SAPS II, SOFA) [131]. Inflammatory cytokines and oxidative stress released during sepsis are high in septic patients, and their concentrations have some association with the severity and evolution of organ dysfunctions [132]. Decreased plasma selenium levels are found to be associated with excess mortality [133]. Plasma selenium concentrations in all patients with sepsis and septic shock are determined to be low (from 0.20 to 0.72 mcmol/l) [134].
Based on the understanding of the main mechanisms of selenium action—suppression of hyperactivation of NF-kB; reduction of activation of the complement system; immunomodulation and anti-inflammatory effect; maintenance of utilization of peroxides; suppression endothelial adhesion (decreased expression of E-selectin, P-selectin); protection of the endothelium from oxygen radicals (using selenoprotein P, which prevents the formation of peroxynitrite from O2 and NO) [129, 135], one can safely assume the expediency of using selenium-containing drugs in complex therapy of SAE to prevent the development of neurocognitive deficiency due to the mechanisms of neuroinflammation in the future [124].
8. Conclusion
The role of selenium in metabolic processes and the importance of correcting its level in various diseases and critical conditions are widely covered in modern literature [40, 43, 44, 45, 46, 47, 48, 50, 70, 135]. Selenium deficiency, which occurs during the development of oxidative stress due to severe TBI, sepsis, and other critical conditions, significantly affects the work of antioxidant systems, reduces the protective mechanisms of the patient’s body and requires correction.
The results of studies of selenium homeostasis in
We are confident that the importance of selenium deficiency correction in the form of selenium replacement therapy is reflected in the treatment protocols of patients in critical conditions, including acute cerebral injury.
Abbreviation
| ALT | alanine aminotransferase |
| APACHE III | Acute Physiology and Chronic Health Evaluation III score |
| AST | aspartate aminotransferase |
| ATP | adenosine triphosphate |
| BBB | blood-brain barrier |
| DiO2 | Iodothyronine deiodinase 2 |
| FOUR | Full Outline of UnResponsiveness Score |
| HIE | hypoxic-ischemic encephalopathy |
| H2S | hydrogen sulfide |
| ICU | intensive care unite |
| IL-1β | interleukin 1β |
| GCR | glucocorticoid receptors |
| GPX1-6 | glutathione peroxidases 1-6 |
| LDH | lactate dehydrogenase |
| mRNA | mitochondrial ribonucleic acid |
| Na2SeO3 | sodium selenite |
| ROS | reactive oxygen species |
| SAE | sepsis-associated encephalopathy |
| SOFA | Sequential Organ Failure Assessment Score |
| TBI | traumatic brain injury |
| TNF-α | tumor necrosis factor-alpha |
References
- 1.
Chen J, Berry MJ. Selenium and selenoproteins in the brain and brain diseases. Journal of Neurochemistry. 2007; 86 :1-12 - 2.
Rayman MP. The importance of selenium to human health. Lancet. 2000; 356 :233-241 - 3.
Rao L, Puschner B, Prolia TA. Gene expression profiling of low selenium status in the mouse intestine. The Journal of Nutrition. 2001; 131 :3175-3181 - 4.
Vladimirov YA. Free radicals in biological systems. Yu. A. Vladimirov Biology. 2000; 6 (12):13-19 - 5.
Zaichik AS, Churilov LP. General Pathophysiology. St. Petersburg: Albi; 2001. p. 467 - 6.
Yeo JE, Kyung S, Kang SK. Selenium effectively inhibits ROS-mediated apoptotic neural precursor cell death in vitro and in vivo in traumatic brain injury. Journal of Biochimica et Biophysica Acta. 2007; 1772 (11-12):1199-1210 - 7.
Kiymaz N, Ekin S, Yilmaz N. Plasma vitamin E and selenium levels in rats with head trauma. Surgical Neurology. 2007; 68 (1):67-70 - 8.
Ozbal S, Erbil G, Kocdor H, Tugyan K, Pekcetin C, Ozogul C. The effects of selenium against cerebral ischemia-reperfusion injury in rats. Neuroscience Letters. 2008; 438 (3):265-269 - 9.
Naziroglu M, Kutluhan S, Yilmaz M. Selenium and topizamate modulates brain microsomal oxidative stress values, Ca 2+-ATPase activity, and EEG records in pentylentetrazol-induced seizures in rats. The Journal of Membrane Biology. 2012; 225 (1):39-49 - 10.
Dalla Puppa L, Savaskan NE, Bräuer AU, Behne D, Kyriakopoulos A. The role of selenite on microglial migration. Annals of the New York Academy of Sciences. 2007; 1096 :179-183 - 11.
Kaziakhmedov VA. Selenium metabolism in severe TBI pediatric patients. Abstract of the dissertation of a candidate of medical sciences. Saint-Petersburg. 2007:19 - 12.
Savaskan NE, Bräuer AU, Kühbacher M, Eyüpoglu IY, Kyriakopoulos A, Ninnemann O, et al. Selenium deficiency increases susceptibility to glutamate-induced excitotoxicity. The FASEB Journal. 2003; 17 :112-114 - 13.
Hill KE, Zhou J, Austin LM, Motley AK, Ham AJ, Olson GE, et al. The selenium-rich C-terminal domain of mouse selenoprotein P is necessary for the supply of selenium to brain and testis but not for the maintenance of whole body selenium. The Journal of Biological Chemistry. 2007; 282 :10972-10980 - 14.
Scharpf M, Schweizer U, Arzberger T, Roggendorf W, Schomburg L, Kohrle J. Neuronal and ependymal expression of selenoprotein P in the human brain. Journal of Neural Transmission. 2007; 114 :877-884 - 15.
Schomburg L, Schweizer U, Holtmann B, Flohe L, Sendtner M, Kohrle J. Gene disruption discloses role of selenoprotein P in selenium delivery to target tissues. The Biochemical Journal. 2003; 370 :397-402 - 16.
Burk RF, Hill KE. Selenoprotein P-expression, functions, and roles in mammals. Biochimica et Biophysica Acta. 2009; 1790 (11):1441-1447 - 17.
Torres DJ, Alfulaij N, Berry MJ. Stress and the brain: An emerging role for selenium. Frontiers in Neuroscience. 2021; 15 :666601. DOI: 10.3389/fnins.2021.666601 - 18.
Solovyev ND. Importance of selenium and selenoprotein for brain function: From antioxidant protection to neuronal signalling. Journal of Inorganic Biochemistry. 2015; 153 :1-12 - 19.
Nakashidze I, Chikovani T, Sanikidze T, Bakhutashvili V. Manifestations of oxidative stress and its correction in traumatic shock. Anesthesiology and resuscitation. 2003; 5 :22-24 - 20.
Alonso de Vega JM, Diaz J, Serrano E, Carbonell LF. Oxidative stress in critically ill patients with systemic inflammatory response syndrome. Critical Care Medicine. 2002; 30 :1782-1786 - 21.
Motoyama T, Okamoto K, Kukita I, Hamaguchi M, Kinoshita Y, Ogawa H. Possible role of increased oxidant stress in multiple organ failure after systemic inflammatory response syndrome. Critical Care Medicine. 2003; 31 :1048-1052 - 22.
Avenell A, Noble DW, Barr J, Engelhardt T. Selenium supplementation for critically Ill adults. Anesthesia and Analgesia. 2005; 100 (5):1536-1536 - 23.
Aleksandrovich YS, Kaziakhmedov VA, Arutsova IY, Pshenisnov KV, Korchagin IV. Dynamics of changes in selenium concentration in plasma, urine and erythrocytes in children with severe traumatic brain injury. Anesthesiology and Resuscitation. 2008; 1 :23-26 - 24.
Huang Z, Rose AH, Hoffmann PR. The role of selenium in inflammation and immunity: From molecular mechanisms to therapeutic opportunities. Antioxidants & Redox Signaling. 2012; 16 (7):705-743 - 25.
Sakr Y, Reinhart K, Bloos F, Marx G, Russwurm S, Bauer M, et al. Time course and relationship between plasma selenium concentrations, systemic inflammatory response, sepsis, and multiorgan failure. British Journal of Anaesthesia. 2007; 98 (6):775-784 - 26.
Andrews P. Selenium and glutamine supplements: Where are we heading? A critical care perspective. Current Opinion in Clinical Nutrition and Metabolic Care. 2010; 13 :192-197 - 27.
Andrews PJD, Avenell A, Noble DW, Campbell MK, Croal BL, Simpson WG, et al. Randomised trial of glutamine, selenium, or both, to supplement parenteral nutrition for critically ill patients. BMJ. 2011; 342 :d1542. DOI: 10.1136/bmj.d1542 - 28.
Berger MM. Antioxydant micronutrients in major trauma and burns: Evidence and practice. Nutrition in Clinical Practice. 2006; 21 (5):438-449 - 29.
Tutelyan VA, Knyazhev VA, Khotimchenko SA, Golubkina NA, Kushlinsky NE, Sokolov YA. Selenium in the Human Body. Moscow: RAMS Publishing House; 2002. p. 219 - 30.
Maehira F, Miyagi I, Eguchi Y. Selenium regulates transcription factor NF-kB activation during the acute phase reaction. Clinica Chimica Acta. 2003; 334 :163-171 - 31.
Geoghegan M, McAnley D, Eaton S, Powell-Tuck J. Selenium in critical illness: Current opinion. Critical Care. 2006; 12 (2):136-141 - 32.
Angstwurm MW, Schottdorf J, Schopohl J, Gaertner R. Selenium replacement in patients with severe systemic inflammatory response syndrome improves clinical outcome. Critical Care Medicine. 1999; 27 :1807-1813 - 33.
Angstwurm MW. Practicalities of selenium supplementation in critically ill patients. Current Opinion in Clinical Nutrition and Metabolic Care. 2006; 9 (3):233-238 - 34.
Angstwurm MW, Engelmann L, Zimmermann T, Lehmann C, Spes CH, Abel P, et al. Selenium in intensive care (SIC): Results of a prospective randomized, placebo-controlled, multiple-center study in patients with severe systemic inflammatory response syndrome, sepsis, and septic shock. Critical Care Medicine. 2007; 35 :118-126 - 35.
Manoli I, Alesci S, Blackman MR, Su YA, Rennert OM, Chrousos GP. Mitochondria as key components of the stress response. Trends in Endocrinology and Metabolism. 2007; 18 :190-198 - 36.
Mehta SL, Kumari S, Mendelev N, Li PA. Selenium preserves mitochondrial function, stimulates mitochondrial biogenesis, and reduces infarct volume after focal cerebral ischemia. BMC Neuroscience. 2012; 13 :79 - 37.
Mendelev N, Mehta SL, Witherspoon S, He Q , Sexton JZ, Li PA. Upregulation of human selenoprotein H in murine hippocampal neuronal cells promotes mitochondrial biogenesis and functional performance. Mitochondrion. 2011; 11 :76-82 - 38.
Forceville X. Effects of high doses of selenium, as sodium selenite, in septic shock patients a placebocontrolled, randomized, double-blind, multi-center phase II study-selenium and sepsis. Journal of Trace Elements in Medicine and Biology. 2007; 21 (Suppl 1):62-65 - 39.
Forceville X, Laviolle B, Annane D, Vitoux D, Bleichner G, Korach JM, et al. Effects of high doses of selenium, as sodium selenite, in septic shock: A placebo controlled, randomized, double-blind, phase II study. Critical Care. 2007; 11 :R73 - 40.
Vincent JL, Forceville X. Critically elucidating the role of selenium. Current Opinion in Anaesthesiology. 2008; 21 :148-154 - 41.
Gelfand BR, Yakovleva II, Popov TV, Glushko AV. Experience of using the drug Selenase in the intensive care complex of patients with destructive pancreatitis. Infections in Surgery. 2008; 1 :54-56 - 42.
Wang Z, Forceville X, Van Antwerp P, Piagnerelli M, Ahishakiye D, Macours P, et al. A large bolus, but not a continuous infusion, of sodium selenite improves outcome in peritonitis. Shock. 2009; 32 :140-146 - 43.
Manzanares W, Biestro A, Torre MH, Galusso F, Facchin G, Hardy G. High-dose selenium reduces ventilator-associated pneumonia and illness severity in critically ill patients with systemic inflammation. Intensive Care Medicine. 2011; 37 :1120-1127 - 44.
Manzanares W, Biestro A, Torre MH, Galusso F, Forre MN, Manay N, et al. Serum selenium and glutathion peroxidase-3 activity: biomarkers of systemic inflammation in the critically ill. Intensive Care Medicine. 2009; 35 :882-889 - 45.
Manzanares W, Hardy G. Selenium supplementation in the critically ill. Phisiology and pharmacokinetics. Current Opinion in Clinical Nutrition and Metabolic Care. 2009; 12 :273-280 - 46.
Manzanares W., Biestro A., Galusso F. et al. Serum selenium and glutationeperoxidase-3 activity biomarkers of systemic inflammation in the critically ill. Intensive Care Medicine. 2009; 35. p. 882-889 - 47.
Manzanares W, Biestro A, Torre MH, Galusso F, Facchın G, Hardy G. Clinical effects of high dose selenious acid in critically ill patients with systemic inflammation. Journal of Parenteral and Enteral Nutrition. 2009; 33 :186 - 48.
Manzanares W, Biestro A, Torre MH, Galusso F, Forre MN, Manay N, et al. High-dose selenium for critically ill patients with systemic inflammation: A pilot study. Nutrition. 2010; 26 :634-640 - 49.
Tinggi U. Selenium: Its role as antioxidant in human health. Environmental Health and Preventive Medicine. 2008; 13 :102-108 - 50.
Matthias WA, Angstwurm MW, Engelmann L, Zimmermann T, et al. Selenium in Intensive Care (SIC) study: Results of a prospective randomized, placebo-controlled, multiple-center study in patients with severe systemic inflammatory response syndrome, sepsis, and septic shock. Critical Care Medicine. 2007; 35 (1):1-8 - 51.
Koszta G, Kacska Z, Szatmari K, Szerafin T, Fulesdi B. Lower whole blood selenium level is associated with higher operative risk and mortality following cardiac surgery. Journal of Anesthesia. 2012; 26 :812-821 - 52.
Forceville X, Van Antwerpen P, Annane D, Vincent JL. Selenocompounds and Sepsis-Redox bypass hypothesis: Part B-Selenocompounds in the management of early Sepsis. Antioxidants & Redox Signaling. 2022; 37 (13-15):998-1029 - 53.
Gao Y, Wang Z, Li Y, Yang J, Liao Z, Liu J, et al. A rational design of copper–selenium nanoclusters that cures sepsis by consuming endogenous H2S to trigger photothermal therapy and ROS burst. Biomaterials Science. 2022; 10 (12):3137-3157 - 54.
Lehmann C, Egerer K, Weber M, Krausch D, Wauer H, Newie T, et al. Effect of selenium administration on various laboratory parameters of patients at risk for sepsis syndrome. Medizinische Klinik. 2007; 15 (Suppl. 3):14-16 - 55.
Shenkin A. Selenium in intravenous nutrition. Gastroenterology. 2009; 137 :S61-S69 - 56.
Singer P, Berger MM, Van den Berghe G, Biolo G, Calder P, Forbes A, et al. ESPEN Guidelines on parenteral nutrition: Intensive care. Clinical Nutrition. 2009; 28 :387-400 - 57.
Bozzetti F, Forbes A. The ESPEN clinical practice guidelines on parenteral nutrition: present status and perspectives for future research. Clinical Nutrition. 2009; 28 :359-364 - 58.
Rupinder D, Naomi C, Margot L, Daren KH. The Canadian critical care nutrition guidelines in 2013: An update on current recommendations and implementation strategies. Nutrition in Clinical Practice. 2014; 29 (1):29-43. doi: 10.1177/0884533613510948 - 59.
von Gagern G, Zimmermann T, Albrecht S, et al. Significance of selenium in regulation of inflammatory response b transcription factors in polytrauma patients. A clinical study. Medizinische Klinik. 1999; 15 (Suppl 3):62-65 - 60.
Nazarov RV, Tsentsiper LM, Kondratieva EA, Kondratiev SA, Semenov EL, Dryagina NV. The place and role of selenium in the correction of systemic inflammatory response of patients in prolonged unconsciousness. Efferent Therapy. 2011; 17 (3):100-101 - 61.
Chelkeba L, Ahmadi A, Abdollahi M, et al. The effect of parenteral selenium on outcomes of mechanically ventilated patients following sepsis: A prospective randomized clinical trial. Annals of Intensive Care. 2015; 5 :29. DOI: 10.1186/s13613-015-0071-y - 62.
Landesberg G, Levin PD, Gilon D, et al. Disfunção miocárdica em sepse grave e choque séptico—sem correlação com citocinas inflamatórias em ambiente clínico da vida real. Baú. 2015; 148 (1):93-102 - 63.
Kieliszek M, Lipinski B. Selenium supplementation in the prevention of coronavirus infections (COVID-19). Medical Hypotheses. 2020; 143 :109878. DOI: 10.1016/j.mehy.2020.109878 - 64.
Mahmoodpoor A, Hamishehkar H, Sanaie S, et al. Antioxidant reserve of the lungs and ventilator-associated pneumonia: A clinical trial of high dose selenium in critically ill patients. Journal of Critical Care. 2018; 44 :357-362. DOI: 10.1016/j.jcrc.2017.12.016 - 65.
Huang JF, Hsu CP, Ouyang CH, Cheng CT, Wang CC, Liao CH, et al. The impact of selenium supplementation on trauma patients-systematic review and Meta-analysis. Nutrients. 2022; 14 (2):342 - 66.
Kong L, Wu Q , Liu B. The impact of selenium administration on severe sepsis or septic shock: A meta-analysis of randomized controlled trials. African Health Sciences. 2021; 21 (1):277-285 - 67.
Manzanares W, Dhaliwal R, Jiang X, Murch L, Heyland DK. Antioxidant micronutrients in the critically ill: A systematic review and meta-analysis. Critical Care. 2012; 16 (2):R66 - 68.
Valenta J, Brodska H, Drabek T, Hendl J, Kazda A. High-dose selenium substitution in sepsis: A prospective randomized clinical trial. Intensive Care Medicine. 2011; 37 (5):808-815 - 69.
Zhang X, Liu RP, Cheng WH, Zhu JH. Prioritized brain selenium retention and selenoprotein expression: Nutritional insights into Parkinson's disease. Mechanisms of Ageing and Development. 2019; 180 :89-96 - 70.
Solovyev N, Drobyshev E, Bjørklund G, Dubrovskii Y, Lysiuk R, Rayman MP. Selenium, selenoprotein P, and Alzheimer’s disease: Is there a link? Free Radical Biology & Medicine. 2018; 127 :124-133 - 71.
de Toledo JHDS, de TF Fraga Silva C, Borim PA, de Oliveira LRC, da Oliveira ES, Périco LL. Organic selenium reaches the central nervous system and downmodulates local inflammation: A complementary therapy for multiple sclerosis? Frontiers in Immunology. 2020; 11 :571844 - 72.
Alim I, Caulfield JT, Chen Y, Swarup V, Geschwind DH, Ivanova E, et al. Selenium drives a transcriptional adaptive program to block ferroptosis and treat stroke. Cell. 2019; 177 (5):1262-1279.e25 - 73.
Meseguer I, Molina JA, Jimenez-Jimenez FJ, et al. Cerebrospinal fluid levels of selenium in patients with Alzheimer's disease. Journal of Neural Transmission. 1999; 106 :309-315 - 74.
Gao S, Jin Y, Hall KS, Liang C, Unverzagt FW, Ji R, et al. Selenium level and cognitive function in rural elderly Chinese. American Journal of Epidemiology. 2007; 165 :955-965 - 75.
Thiel R, Fowkes SW. Can cognitive deterioration associated with Down syndrome be reduced? Medical Hypotheses. 2005; 64 (3):524-532 - 76.
Zafar KS, Siddiqui A, Sayeed I, Ahmad M, Salim S, Islam F. Dose-dependent protective effect of selenium in rat model of Parkinson's disease: Neurobehavioral and neurochemical evidences. Journal of Neurochemistry. 2003; 84 :438-446 - 77.
Aguilar MV, Jimenez-Jimenez FJ, Molina JA, et al. Cerebrospinal fluid selenium and chromium levels in patients with Parkinson's disease. Journal of Neural Transmission. 1998; 105 :1245-1251 - 78.
Kim H, Jhoo W, Shin E, Bing G. Selenium deficiency potentiates methamphetamine-induced nigral neuronal loss; comparison with MPTP model. Brain Research. 2000; 862 :247-252 - 79.
Kim HC, Jhoo WK, Choi DY, Im DH, Shin EJ, Suh JH, et al. Protection of methamphetamine nigrostriatal toxicity by dietary selenium. Brain Research. 1999; 851 :76-86 - 80.
Steinbrenner H, Alili L, Bilgic E, Sies H, Brenneisen P. Involvement of selenoprotein P in protection of human astrocytes from oxidative damage. Free Radical Biology & Medicine. 2006; 40 :1513-1523 - 81.
Ashrafi MR, Shams S, Nouri M, Mohseni M, Shabanian R, Yekaninejad MS, et al. A probable causative factor for an old problem: Selenium and glutathione peroxidase appear to play important roles in epilepsy pathogenesis. Epilepsia. 2007; 13 :1256-1268 - 82.
Nazıroğlu M, Yürekli VA. Effects of antiepileptic drugs on antioxidant and oxidant molecular pathways: Focus on trace elements. Cellular and Molecular Neurobiology. 2013; 33 (5):589-599 - 83.
Hardy G, Hardy I. Selenium: The Se-XY nutraceutical. Nutrition. 2004; 20 :590-593 - 84.
Zimmermann C, Winnefeld K, Streck S, Roskos MM, Haberl RL. Antioxidant status in acute stroke patients and patients at stroke risk. European Neurology. 2004; 51 (3):157-161. DOI: 10.1159/000077662 - 85.
Ansari MA, Ahmad AS, Ahmad M, Salim S, Yousuf S, Ishrat T, et al. Selenium protects cerebral ischemia in rat brain mitochondria. Biological Trace Element Research. 2004; 101 :73-86 - 86.
Arakawa M, Yoshihiso I. N-acetylcysteine and neurodegenerative diseases: Basic and clinical pharmacology. Cerebellum. 2007; 6 (4):308-314 - 87.
Yousuf S, Atif F, Ahmad M, Hoda MN, Khan MB, Ishrat T, et al. Selenium plays a modulatory role against cerebral ischemia-induced neuronal damage in rat hippocampus. Brain Research. 2007; 1147 :218-225 - 88.
Wray JR, Davies A, Sefton C, Allen TJ, Adamson A, Chapman P, et al. Global transcriptomic analysis of the arcuate nucleus following chronic glucocorticoid treatment. Molecular Metabolism. 2019; 26 :5-17 - 89.
Perez A, Jansen-Chaparro S, Saigi I, Bernal-Lopez MR, Miñambres I, Gomez-Huelgas R. Glucocorticoid-induced hyperglycemia. Journal of Diabetes. 2014; 6 (1):9-20 - 90.
Saito I, Asano T, Sano K, Takakura K, Abe H, Yoshimoto T, et al. Neuroprotective effect of an antioxidant, ebselen, in patients with delayed neurological deficits after aneurysmal subarachnoid hemorrhage. Neurosurgery. 1998; 42 :269-277 - 91.
Yamaguchi T, Sano K, Takakura K, Saito I, Shinohara Y, Asano T, et al. Ebselen in acute ischemic stroke: A placebo-controlled, double-blind clinical trial. Ebselen Study Group. Stroke. 1998; 29 :12-17 - 92.
Kühbacher M, Bartel J, Hoppe B, Alber D, Bukalis G, Bräuer A, et al. The brain selenoproteome: Priorities in the hierarchy and different levels of selenium homeostasis in the brain of selenium-deficient rats. Journal of Neurochemistry. 2009; 110 :133-142 - 93.
Xu L, Zhang S, Chen W, Yan L, Chen Y, Wen H, et al. Trace elements differences in the depression sensitive and resilient rat models. Biochemical and Biophysical Research Communications. 2020; 529 (2):204-209 - 94.
Pasco JA, Jacka FN, Williams LJ, Evans-Cleverdon M, Brennan SL, Kotowicz MA, et al. Selenium and major depression: A nested case-control study. Complementary Therapies in Medicine. 2012; 20 (3):119-123 - 95.
Burk RF, Hill KE. Selenoprotein P: An extracellular protein with unique physical characteristics and a role in selenium homeostasis. Annual Review of Nutrition. 2005; 25 :215-235 - 96.
Burk RF, Hill KE, Olson GE, Weeber EJ, Motley AK, Winfrey VP, et al. Deletion of apolipoprotein E receptor-2 in mice lowers brain selenium and causes severe neurological dysfunction and death when a low-selenium diet is fed. The Journal of Neuroscience. 2007; 27 :6207-6211 - 97.
Hoffmann PR, Höge SC, An LP, Hoffmann FW, Hashimoto AC, Berry MJ. The selenoproteome exhibits widely varying, tissue-specific dependence on selenoprotein P for selenium supply. Nucleic Acids Research. 2007; 35 (12):3963-3973. DOI: 10.1093/nar/gkm355 - 98.
Erbil G, Ozbal S, Sonmez U, Pekketin C, Tugyan K, Bayriyanik A, et al. Neuroprotective effects of selenium and ginkgo biloba extract (Egb761) against ischemia and reperfusion injury in rat brain. Neurosciences. 2008; 13 (3):233-238 - 99.
Casaril AM, Domingues M, Bampi SR, de Andrade LD, Padilha NB, Lenardão EJ, et al. The selenium-containing compound 3-((4-chlorophenyl)selanyl)-1-methyl-1H-indole reverses depressive-like behavior induced by acute restraint stress in mice: Modulation of oxido-nitrosative stress and inflammatory pathway. Psychopharmacology (Berl). 2019; 236 (10):2867-2880 - 100.
Casaril AM, Ignasiak MT, Chuang CY, Vieira B, Padilha NB, Carroll L, et al. Selenium-containing indolyl compounds: Kinetics of reaction with inflammation-associated oxidants and protective effect against oxidation of extracellular matrix proteins. Free Radical Biology & Medicine. 2017; 113 :395-405 - 101.
Casaril AM, Domingues M, Fronza M, Vieira B, Begnini K, Lenardão EJ, et al. Antidepressant-like effect of a new selenium-containing compound is accompanied by a reduction of neuroinflammation and oxidative stress in lipopolysaccharide-challenged mice. Journal of Psychopharmacology (Oxford, England). 2017; 31 (9):1263-1273 - 102.
Yeo JE, Kim JH, Kang SK. Selenium attenuates ROS-mediated apoptotic cell death of injured spinal cord through prevention of mitochondria dysfunction; in vitro and in vivo study. Cellular Physiology and Biochemistry. 2008; 21 :225-238 - 103.
Yin W, Signore AP, Iwai M, Cao G, Gao Y, Chen J. Rapidly increased neuronal mitochondrial biogenesis after hypoxic-ischemic brain injury. Stroke. 2008; 39 :3057-3063 - 104.
Zhou YJ, Zhang SP, Liu CW, Cai YQ. The protection of selenium on ROS mediated-apoptosis by mitochondria dysfunction in cadmium-induced LLC-PK(1) cells. Toxicology In Vitro. 2009; 23 :288-294 - 105.
Schweizer U, Brauer AU, Kohrle J, Nitsch R, Savaskan NE. Selenium and brain function: a poorly recognized liaison. Brain Research. Brain Research Reviews. 2004; 45 :164-178 - 106.
Schweizer U, Schomburg L. Selenium, selenoproteins and brain function. In: Hatfield DL, Berry MJ, Gladyshev VN, editors. Selenium its Molecular Biology and Role in Human Health. US: Springer; 2004. pp. 233-248 - 107.
Wang Q , Zhang QG, Wu DN, Yin XH, Zhang GY. Neuroprotection of selenite against ischemic brain injury through negatively regulating early activation of ASK1/JNK cascade via activation of PI3K/AKT pathway. Acta Pharmacologica Sinica. 2007; 28 :19-27 - 108.
Sarada SK, Himadri P, Ruma D, Sharma SK, Pauline T. Mrinalini: Selenium protects the hypoxia induced apoptosis in neuroblastoma cells through upregulation of Bcl-2. Brain Research. 2008; 1209 :29-39 - 109.
Peters MM, Hill KE, Burk RF, Weeber EJ. Altered hippocampus synaptic function in selenoprotein P deficient mice. Molecular Neurodegeneration. 2006; 1 :12 - 110.
Wirth EK, Conrad M, Winterer J, Wozny C, Carlson BA, Roth S, et al. Neuronal selenoprotein expression is required for interneuron development and prevents seizures and neurodegeneration. The FASEB Journal. 2010; 24 :844-852 - 111.
Leiter O, Zhuo Z, Rust R, Wasielewska JM, Gronnert L, Kowal S, et al. Selenium mediates exercise-induced adult neurogenesis and reverses learning deficits induced by hippocampal injury and aging. Cell Metabolism. 2022; 34 :408-423 - 112.
Yao H, Zhao X, Fan R, Sattar H, Zhao J, Zhao W, et al. Selenium deficiency-induced alterations in ion profiles in chicken muscle. PLoS One. 6 Sep 2017; 12 (9):e0184186. doi: 10.1371/journal.pone.0184186 - 113.
Yang B, Li Y, Ma Y, Zhang X, Yang L, Shen X, et al. Selenium attenuates ischemia/reperfusion injury-induced damage to the blood-brain barrier in hyperglycemia through PI3K/AKT/mTOR pathway-mediated autophagy inhibition. International Journal of Molecular Medicine. 2021; 48 (3):1-13 - 114.
Ataizi ZS, Ertilav K, Nazıroğlu M. Mitochondrial oxidative stress-induced brain and hippocampus apoptosis decrease through modulation of caspase activity, Ca2+ influx and inflammatory cytokine molecular pathways in the docetaxel-treated mice by melatonin and selenium treatments. Metabolic Brain Disease. 2019; 34 (4):1077-1089 - 115.
Khalili H, Ahl R, Cao Y, Paydar S, Sjölin G, Niakan A, et al. Early selenium treatment for traumatic brain injury: Does it improve survival and functional outcome? Injury. 2017; 48 (9):1922-1926 - 116.
Savvina IA. Effective criteria of selenium therapy in patients with brain injury. I.A. Savvina, H.S. Nucalova. 6 th International Baltic Congress Anaesthesiology Intensive Care. Acta Medica Lituanica. 2012; 19 (3):391 - 117.
Savvina, I.A. Selenium therapy controls the oxidative stress level in patients with traumatic brain injury. I.A. Savvina, H.S. Nucalova, M. D. Astaeva 32 nd Congress of the Scandinavian Society of Anaesthesiology and Intensive Care Medicine. Acta Anaesthesiologica Scandinavica. 2013; 57 (Suppl. 120):30 - 118.
Nutsalova HS, Mishina TP, Savvina IA. Dynamics of some clinical and laboratory indicators of systemic inflammatory response in patients with severe traumatic brain injury depending on the intake of selenium-containing drugs. Emergency Medical Help. 2014; 15 (2):60-64 - 119.
Nutsalova HS. Selenium replacement therapy in severe TBI patients. Abstract of the dissertation of a candidate of medical sciences. Makhachkala: Dzhamaludinov Publisher House; 2014. p. 24 - 120.
Moghaddam OM, Lahiji MN, Hassani V, Mozari S. Early administration of selenium in patients with acute traumatic brain injury: A randomized double-blinded controlled trial. Indian Journal of Critical Care Medicine: Peer-reviewed, Official Publication of Indian Society of Critical Care Medicine. 2017; 21 (2):75-79 - 121.
Hirato J, Nakazato Y, Koyama H, Yamada A, Suzuki N, Kuroiwa M, et al. Encephalopathy in megacystis-microcolon-intestinal hypoperistalsis syndrome patients on long-term total parenteral nutrition possibly due to selenium deficiency. Acta Neuropathol (Berl). 2003; 106 (3):234-242 - 122.
Abdel-Azeem M. El-Mazary, Reem A. Abdel-Aziz, Ramadan A. Mahmoud, Mostafa A. El-Said & Nashwa R. Mohammed correlations between maternal and neonatal serum selenium levels in full term neonates with hypoxic ischemic encephalopathy. Italian Journal of Pediatrics. 2015; 41 :83 - 123.
Aggarwal R, Gathwala G, Yadav S, Kumar P. Selenium supplementation for prevention of late-onset Sepsis in very low birth weight preterm neonates. Journal of Tropical Pediatrics. 2016; 62 (3):185-193 - 124.
Bykova KM, Savvina IA, Zabrodskaya YM, Bodareva NV. Pathophysiological aspects and complex diagnostics of sepsis-associated encephalopathy. Perspectives of etiopathogenetic therapy. Anesthesiology and Reanimatology. 2022; 4 :92-98 - 125.
Sonneville R, Verdonk F, Rauturier C, et al. Understanding brain dysfunction in sepsis. Annals of Intensive Care. 2013; 3 :15 - 126.
Haruwaka K, Ikegami A, Tachibana Y, et al. Dual microglia effects on blood brain barrier permeability induced by systemic inflammation. Nature Communications. 2019; 10 :5816. DOI: 10.1038/s41467-019-13812-z - 127.
Erickson MA, Banks WA. Neuroimmune axes of the blood-brain barriers and blood-brain interfaces: Bases for physiological regulation, disease states, and pharmacological interventions. Pharmacological Reviews. 2018; 70 :278-314 - 128.
Wang H, Wang H, Song Y, et al. Overexpression of Foxc1 ameliorates sepsis associated encephalopathy by inhibiting microglial migration and neuroinflammation through the IκBα/NFκB pathway. Molecular Medicine Reports. 2022; 25 :107 - 129.
Solovyev N, Drobyshev E, Blume B, Michalke B. Selenium at the neural barriers: A review. Frontiers in Neuroscience. 2021, 2021; 15 :630016. DOI: 10.3389/fnins.2021.630016 - 130.
Xie Z, Xu M, Xie J, et al. Inhibition of ferroptosis attenuates glutamate excitotoxicity and nuclear autophagy In a CLP septic mouse model. Shock Augusta Ga. 2022; 70 :278 - 131.
Savvina IA, Ryzhkova DV, Bykova KM, Lebedev KE, Petrova AO, Dryagina NV, et al. Diagnostics of central and autonomic nervous system dysfunction in patients with Sepsis-associated encephalopathy. In: Huang L, Zhang Y, Sun L, editors. Sepsis New Perspectives. London: IntechOpen; 2022. DOI: 10.5772/intechopen.108392. Available from: https://www.intechopen.com/online-first/diagnostics-of-central-and-autonomic-nervous-system-dysfunction-in-patients-with-sepsis-associated-e - 132.
Eidt MV, Nunes FB, Pedrazza L, Caeran G, Pellegrin G, Melo DA, et al. Biochemical and inflammatory aspects in patients with severe sepsis and septic shock: The predictive role of IL-18 in mortality, Clinica chimica acta. International Journal of Clinical Chemistry. 2016; 453 :100-106 - 133.
Jang JY, Shim H, Lee SH, Lee JG. Serum selenium and zinc levels in critically ill surgical patients. Journal of Critical Care. 2014; 29 (2):317-318 - 134.
Forseville X, Vitox D, Gauzitetal R. Selenium, systemic immune response syndrome, sepsis, and outcome in critically ill patients. Critical Care Medicine. 1998; 26 (9):1536-1544 - 135.
Panee J, Liu W, Nakamura K, Berry MJ. The responses of HT22 cells to the blockade of mitochondrial complexes and potential protective effect of selenium supplementation. International Journal of Biological Sciences. 2007; 3 :335-341