
Abstract
Regenerative medicine aims to repair organs or tissues that have congenital abnormalities, or that have been damaged by disease, aging, or trauma, and to restore or at least improve their native function. One of the strategies used in regenerative medicine is stem cell therapy, due to the enormous regenerative potential of stem cells. A staminal cell line is a group of cells that can replicate for an extended period in vitro, that is outside the body. These cells are grown in incubators using a culture medium that should have a temperature and an oxygen/carbon dioxide composition that simulates the desired environment. This chapter describes the main characteristics of stem cells, the main fields of application, and outlines what could be the future developments of their use, also considering the ethical and technical problems that currently limit their use. There is still much to be done in the field of stem cell research, and researchers are working tirelessly to remain leaders and innovators in it. A struggle, step by step, will make it possible to have more information on current knowledge by expanding the scientific literature and push current limits ever further.
Keywords
- stem cells
- regenerative medicine
- clinical studies
- research strategies
- therapeutic method
1. Introduction
In recent years, increasing attention has been paid to the study of various types of cells, with particular attention to their properties, to promote regenerative processes and/or to be used for the cellular treatment of many diseases [1]. Great interest in research has been aroused by stem cells; their ability to self-renew, and differentiate into mature adult cells has made them, since their discovery, extremely promising for the regeneration of human tissue [2]. It is no coincidence that the first results of their use have contributed to the real definition of “regenerative medicine” [3]. Today, stem cells and their differentiated derivates are increasingly used in an ever-widening field of cellular studies, often with the aim of treating the condition of cell loss related to various diseases [4].
Stem cell division can give birth to an asymmetrical offspring with an additional progenitor cell and a daughter stem cell. For this reason, they exhibit both self-renewal and regeneration capabilities. The differentiation capacity of stem cells depends on their specification potential.
Generally, the renewal of adult stem cells (ASCs) is limited because they can only differentiate into specific cells of a single tissue. Finding stem cells capable of differentiating into all tissue types is a challenge. In the event that all terminal cell populations can be reached the cells are said to have the property of totipotency, while the ability to pursue a more restricted pattern of phenotypes is the property of multipotency [5] (Figure 1).
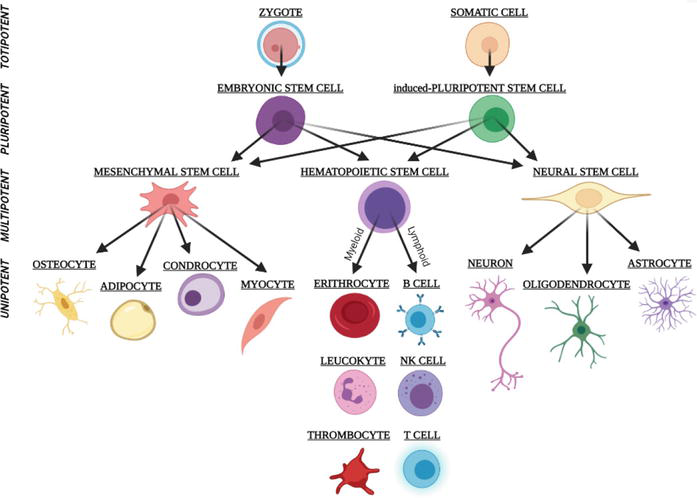
Figure 1.
Totipotent stem cells generate all the cell types of the organism (e.g., zygote or fertilized egg). Pluripotent stem cells produce all the embryonic germ layers (endoderm, ectoderm, and mesoderm). Multipotent stem cells generate a limited number of cell types based on their tissue of origin. Mesenchymal stem cells give rise to fat, bone, muscle, and cartilage. Hematopoietic stem cells give rise to different types of blood cells (for example platelets, and red and white cells). Neural stem cells give rise to neurons, oligodendrocytes, and astrocytes. Oligopotent stem cells generate some closely related cell types (for example myeloid stem cells). Unipotent stem cells generate a single cell type (e.g., epidermal stem cells or muscle stem cells) [
Scientists have traditionally dealt with two types of animal and human stem cells: embryonic stem cells (ESCs) and non-embryonic “somatic” or “adult” stem cells. Almost 30 years ago, in 1981, researchers discovered how to obtain ESCs from early mouse embryos [7]. A method to extract stem cells from human embryos, and growing the cells in the laboratory was discovered in 1998, as a result of a deepen examination of mouse stem cell biology [8]. Human embryonic stem cells (hESCs) were the name given to these cells. The
A possible way to overcome this obstacle was already found in 2006 by Takahashi and Yamanaka. Under unknown circumstances, some specialized adult cells were genetically “reprogrammed” to take on a stem cell-like form. The current name of this novel form of stem cell is induced pluripotent stem cell (iPSCs). iPSCs exhibit morphology, growth properties, and cell marker gene expression of ESCs, without ethical concerns. iPSCs can differentiate in various human tissues and exploit regenerate properties [11, 12], given their pluripotency capability. Unlike hESCs, iPSCs do not raise any ethical concerns regarding the timing of human personality initiation [13, 14].
However, both ESCs and IPSCs carry the risk of tumor formation, a risk related to both pluripotency and self-renewal. This is a critical factor of both cells types [15]. Furthermore, iPSCs still present some technical issues related to immune rejection after transplantation. This means that research in this field needs to be expanded because more studies are needed before using iPSCs as a viable tool for
2. Origin of stem cells
Stem cells have the ability to self-renew, i.e. to create copies of themselves, and to differentiation into lineage populations, i.e. to develop into more specialized cells, which allow cell turnover in the respective tissues present in multicellular organisms [18]. The production of tissue-specific stem cells, which generally assist the cell renewal of all tissue types for the development of the organism, is a necessary step in the life cycle of a complex organism [19].
The core cells of the 3- to 5-day-old embryo, known as blastocysts, give rise to the complete body of an organism, including the numerous specialized cell types and organs such as the heart, lung, skin, sperm, eggs, and other tissues [20].
Distinct populations of ASCs provide replacements for cells lost due to natural wear and tear, injury, or disease in different adult tissues, such as bone marrow, muscle, and brain. Stem cells allow novel therapeutic possibilities for addressing these conditions thanks to their exceptional ability to regenerate [21].
Scientists can study the basic characteristics of stem cells and what distinguishes them from other specialized cell types through laboratory investigations. In laboratories, stem cells are already being used by researchers to test new drugs, create models/systems to study healthy growth, and pinpoint the origins of birth abnormalities. Understanding of how an organism grows from a single cell and how healthy cells replace damaged ones in adult creatures has been advanced through stem cell research [19, 22].
One of the most promising areas of modern biology is stem cell biological product research. It has recently been ascertained that miRNA-containing vesicles, such as exosomes, could induce a change in some pathologies [23, 24, 25] (Figure 2).
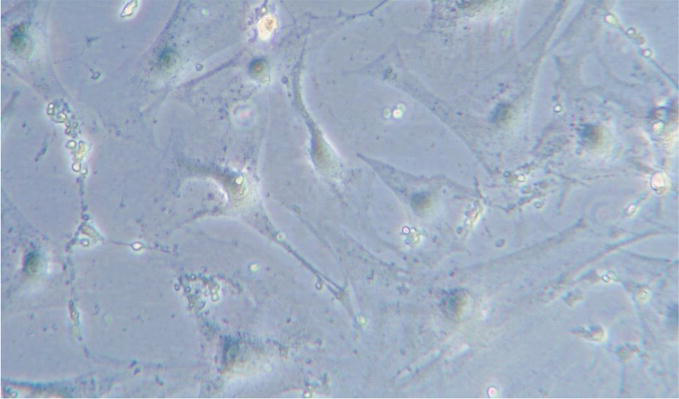
Figure 2.
Adult adipose tissue derived murine stem cells ADAS. Here shown, ADAS cultured with complete DMEM containing 10% FBS and 1% P/S mix 1:1, and incubated at 37°C in a 5% CO2 atmosphere. These cells have the characteristic of producing exosomes, which in recent studies have shown to have unique characteristics for some neuropathologies [
There is still much work to be done in laboratories and clinics to improve the efficacy of using these cells and their byproducts in what are termed cellular treatments, or even regenerative or reparative medicine treatments, of a diverse pool of diseases [26].
3. Stem cells subpopulations
All stem cells can self-renew and develop, as described in the previous chapter, but they differ greatly in what they can and cannot become and in the conditions under which they can and cannot perform certain functions. This is one reason why scientists employ different kinds of stem cells in their study.
3.1 Adult stem cells
ASCs are undifferentiated cells found in some differentiated tissues of the body and have the possible property of self-renewing or producing new cells to replace damaged or dead tissue [27]. Alternatively, ASCs are sometimes referred to as “somatic stem cells”, where the term “somatic” refers to the non-reproductive cells of the body (eggs or sperm). Some examples of ASCs are: Epithelial and Skin Stem Cells, Neural Stem Cells, Hematopoietic Stem Cells (Blood Stem Cells), Mesenchymal Stem Cells [28] (Figure 3).
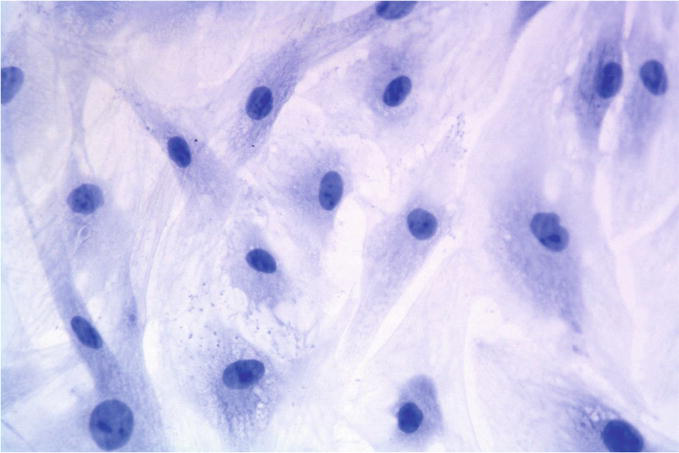
Figure 3.
Fat harvesting via liposuction. Here shown, human adipose derived mesenchymal stem cells cultured with DMEM complete medium for 2 weeks, fixed with PFA 3%, washed PBS 1x stained with hematoxylin, the protocol involved the seeding of ADSCs on a 12-wells plate with sterile slides on the bottom of each well. The cells were seeded and incubated with 1 ml of complete culture medium for 24 hours at 37° C and 5% CO2. At the end the cells were fixed with paraformaldehyde 4%, stained with Mayer’s hematoxylin (bio-Optica, Milan, Italy) for 5 min. Finally, the cells were washed with tap water for 5 min and mounted with mount quick aqueous solution (bio-Optica, Milan, Italy). The image acquisition was done using a bright field optical microscope, Olympus BX-51 (Olympus, Tokyo, Japan) equipped with a digital camera (DKY-F58 CCD JVC, Yokohama, Japan) and connected with a PC endowed with image-pro plus 7.0 software. Slides were gently cleaned with ethanol, acquired using a 20X.
ASCs are often insufficient in native tissues, making them difficult to study and harvest for research [29]. Distinct populations of ASCs, which are present in most tissues in the human body, produce new cells to replace those lost as a result of natural repair, disease, or damage.
All tissues in a person, including the umbilical cord, placenta, bone marrow, muscle, brain, adipose tissue and lipoaspirates, skin, stomach, etc. include ASCs.
In 1948, the first ASCs were removed and utilized to create blood [30]. When the first adult bone marrow cells were employed in clinical therapy for blood disorders in 1968, this process was expanded [31].
For more than 40 years, treatments for blood disorders such as leukemia and lymphoma have included transplantation of peripheral blood stem cell and bone marrow [32].
There is an ongoing debate. According to some studies [33], ASCs can only produce the cell types of the tissue in which they reside. However, other studies suggest that ASCs may be able to produce cells of other tissue types [34]. More research is required to clarify this aspect.
Scientists have demonstrated that ASCs are present in most body tissues. Scientific research is looking for ways to locate, isolate, and multiply these cells for therapeutic use.
Most of the biological effects of ASC are probably mediated by extracellular vesicles, such as exosomes, which influence surrounding cells. The current development of exosome therapies requires efficient and non-invasive methods to localize, monitor, and trace exosomes [25] (Figure 4). The idea behind these therapies is that the exosomes and the chemicals released are the stem cells’ way of manifesting their therapeutic function.
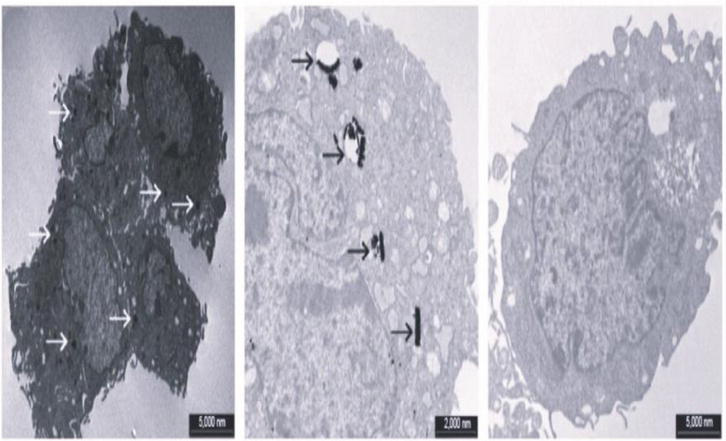
Figure 4.
TEM images of ADAS incubation with nanoparticles (NPs) were morphologically analyzed through a transmission electron microscope (TEM) in order to confirm the intracellular uptake of NPS and visualize their intracellular localization. The scale bar in the left and right pictures is 5000 nm, and the Centre picture is focused on the endocytic invagination containing nanoparticles and the internalized nanoparticles inside the endosome (scale bar 2000 nm). Cell pellets were fixed for 1 h in 2% glutaraldehyde in 0.1 M phosphate buffer (PB) and, after washed, postfixed for 1 h in 1% OsO4 diluted in 0.2 M K3Fe (CN)6. After rinsing in 0.1 M PB, the samples were dehydrated in graded concentrations of acetone and embedded in a mixture of Epon and araldite (electron microscopic sciences, Fort Washington, PA, USA). Ultrathin sections were cut at 70 nm thickness on a Ultracut E ultramicrotome (Reichert-Jung, Heidelberg, Germany), placed on Cu/Rh grids and contrasted with lead citrate. Samples were observed with Pa Philips Morgagni 268 D electron microscope (Fei company, Eindhoven, the Netherlands) equipped with a mega view II camera to acquire digital images [
3.1.1 What are exosomes?
Exosomes are vesicles that include peptides, mRNA, and microRNAs ([35, 36]), range in size from 50 to 150 nm, and are essential for intercellular communication [37]. They mimic the effects of stem cell transplantation by delivering physiologically active chemicals to recipient cells, which change their gene expression and behavior.
According to several studies, stem cell-derived exosomes may have a role in synaptic plasticity, nerve regeneration, neuronal protection, and neurological recovery [38, 39].
By using these vesicles as a treatment, rather than their generated parental cells, restrictions and dangers for cell transplantation are avoided.
3.2 Embryonic stem cells
The embryo, known as a blastocyst at this stage, contains an inner cell mass capable of growing all the specialized tissues that make up the human body, 3 to 5 days after fertilization and prior to implantation [40]. ESCs are produced from the inner cell mass of an
Isolable only in the early stages of development, these pluripotent stem cells can develop into virtually any cellular form (Figure 5). One of the research objectives is to understand how these cells differentiate during development [42]. The progressive increase in knowledge about these stages of development, could allow researchers to use ESCs generated
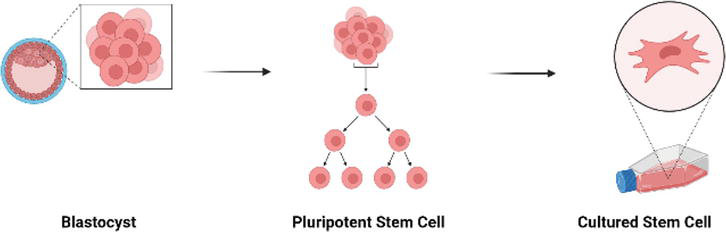
Figure 5.
Schematic representation of ESCs. ESCs are pluripotent, and are derived from the inner cell mass of a blastocyst. Human embryos reach the blastocyst stage 4–5 days after fertilization and at that time consist of approximately 50–150 cells [
In the future, ESCs could be used to treat a broader spectrum of disorders. It is hoped that once this technique is well understood, the information will be applied to vehicular ESCs, i.e., induce them to differentiate into the specific cell type required for patient therapy [44]. Currently, diseases treated with ESCs transplantation include diabetes, spinal cord injury, muscular dystrophy, heart disease, and vision/hearing loss [45].
3.3 Reprogrammed pluripotent stem cells
Halfway between ASCs and ESCs are iPSCs, which are stem cells produced in a laboratory, by introducing embryonic genes into a somatic cell, such as a skin cell, so that it returns to a “stem cell-like” state [46].
The production of these cells is an innovative technique of genetic reprogramming. First identified in 2006 [47], several years of study will be required before they can be used therapeutically.
The potential to alter recipient somatic cells into a “ESC-like” state undoubtedly makes therapies using iPSCs attractive [48]. The cells required for the therapies could be produced using appropriate differentiation processes of these iPSC cells. What makes this technique attractive is that it circumvents the need for lifelong histocompatibility immunosuppression, as is the case with transplanted cells of donor stem cells [49].
iPSC cells are regarded as pluripotent, making them similar to most ESCs. However, unlike for ESCs, manipulation of iPSCs has not been successful in growing the outer layer of an embryonic cell, which is required for the cell to develop into a full human individual [50]. But, iPSC research is rapidly moving towards translational and clinical applications [51].
4. Advantages of different stem cell lineages
It is possible to list some advantages and disadvantages associated with the three distinct stem cell types (ASCs, ESCs, and iPSC) previously described. If we start from the analysis of the disadvantages and ongoing debates on the use of different stem cells, we are immediately redirected towards their advantages.
ASCs – Among the positive characteristics of ASCs is their ability to transdifferentiate and reprogram themselves. Also they are less likely to be rejected when used in transplants [52]. Their efficiency in the therapeutic field has already been proven in numerous clinical applications [53].
ESCs – Among their advantageous properties, ESCs have the potential to be maintained in culture, and to grow even for more than a year. Numerous protocols have been established for their maintenance in culture, protocols that consider the ability of these cells to produce most cell types in the body [54, 55, 56, 57]. There are numerous studies relating to these cells, which appear to be among the most investigated stem cells. A further increase in these studies may lead to more knowledge about how living things develop and thrive.
iPSCs – iPSCs are mostly derived from donor somatic cells. This means that they can be utilized in large quantities, avoiding histocompatibility issues in transplants. These cells have performed well in preclinical drug testing and research/development studies [58, 59, 60]. The definition of the new cellular “reprogramming” procedure, and the new knowledge deriving from it, could be applied to define
The currently best-known cell therapy for the treatment of blood malignancies and other blood problems is bone marrow transplantation, which transplants blood stem cells [61].
Theoretically, Parkinson’s disease, spinal cord damage, stroke, burns, heart disease, Type 1 diabetes, osteoarthritis, rheumatoid arthritis, muscular dystrophy, and liver disease are all possible candidates for stem cell therapy [62]. Additionally, regeneration of the retina using isolated ocular stem cells could one day contribute to the reversal of blindness, providing a potential treatment for distressed or injured eyes [63].
Cell therapy, which replaces unhealthy cells with healthy ones to treat disease, is one potential use of stem cells; it is comparable to organ transplantation, except that the cells rather than the organs are transplanted (Figure 6).
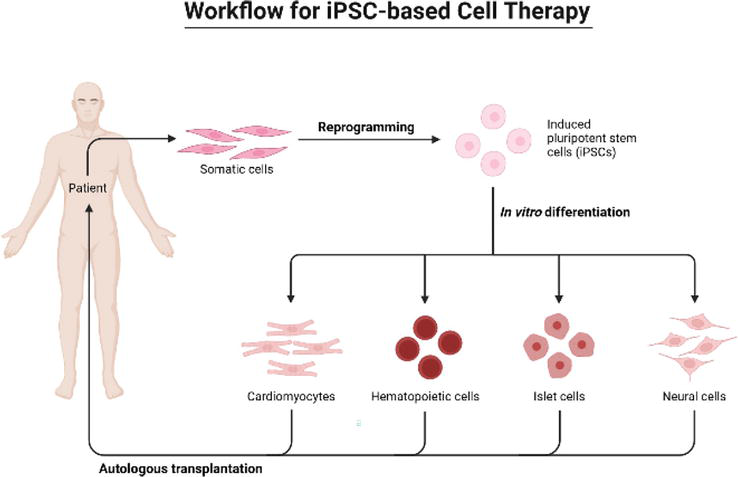
Figure 6.
Autologous human iPSCs can be derived from individual patients and differentiate into different cell types. To develop new therapies, isolated and cultured cells are used to observe specific disease phenotypes and identify possible new pathological mechanisms. Cell therapy includes therapies based on stem and non-stem cells, unicellular and multicellular, with different immunophenotypic profiles, isolation techniques, mechanisms of action and regulatory levels. The use of human iPSCs, autologous to the patient, offers an innovative approach for regenerative medicine ([
5. Limitations and obstacles to their use
Many factors still need to be considered and many studies are still needed to fully understand how to use stem cells.
ASCs – The differentiating capacity of ASCs are not yet fully elucidated [64]. This may mean that a different interpretation of their properties is needed, considering them multi- or unipotent.
Furthermore, ASCs cannot be grown for long periods of time in culture without an observable phenotypic change occurring and fail to prevent their immortalization.
Another limitation of the use of these cells is that they are present in small quantities in the tissues. This makes it difficult to identify the niche and the purification/isolation process is tedious. Currently few technologies are available to generate large quantities of cultured stem cells and keep them incubating. We have previously successfully tested the combination of CELLviewer [65] with Spin∞, a new bioreactor still in the prototype stage [66].
ESCs – The limitations and obstacles that can be found in the use of ESCs concern various aspects, among which the fundamental one is that the cell line generation process is inefficient. Moreover, their use is strictly regulated [67].
It is uncertain whether they would be rejected if used in transplants. Therapies that use ESC pathways are largely new, and much more research and testing is needed to ascertain their effectiveness as alternative pathways to conventional clinical treatments [68].
Finally, when used directly from the undifferentiated culture, ESCs for tissue transplants can generate and cause tumors (teratomas) or the development of cancer.
iPSCs – The reasoning on iPSCS turns out to be more complex. Since the transcription and reprogramming factors of stem cells were identified in 2006 [47], several methods to obtain iPSCs have been certified. These methods have been duly included in protocols that ensure cell reproducibility and maintenance [49]. New discoveries are not uncommon, given that the tissues into which they differentiated are not known
An important limit to the use of these cells are the viruses that are currently used to introduce embryonic genes into somatic cells. Studies in mouse models have shown that these viruses can cause tumors.
The use of iPSCs has given rise to several controversies because, however, there could be numerous application possibilities in the research field and in the market.
As far as ethical aspects are concerned, for the use of ASCs has not raised any significant issue. For the use of ESC, to acquire the inner cell mass, the embryo is destroyed. Therefore, donor consent is required. Relevant problem may concern iPSC cells because, when exposed to the right conditions, they have the potential to become embryos.
It should be noted that there can be many possible hitches related to the cellular therapy. For example, in the presence of insufficient synthesis of stem cells in the bone marrow, a poor transfusion is obtained, i.e. a transfusion with few cells. This is typical of elderly individuals who, compared to younger individuals, have a lower capacity of the bone marrow to produce stem cells. Regardless of the number of cells, the quality of these cells is also crucial.
Finally, not all existing health problem can be solved with stem cell treatment. Each person responds differently; the fundamental goal of this method is to provide the body with the means and the optimal environment to repair damaged tissue on its own. The knowledge of the type of patients to be treated in the different modalities to optimize therapeutic outcomes has significantly improved. For some pathologies/patients, on the other hand, there has been no progress and it is not yet known what the most suitable cell therapy might be. Additionally, the outcome of any procedure relies on the participant’s individual body resilience. Each body can respond differently. Therefore, it is currently not possible to generalize the results of a treatment or to determine it as the ideal treatment for a given pathological condition. There is no universal treatment plan.
6. Future perspectives of culturing stem cells
Faced with the possibility of using different stem cells, it should be remembered that the cells can be used in abundant quantities of donor somatic cells, thus making autologous treatments possible. In other words, the histocompatibility problems typical of transplants from donors other than the recipient, which are normally the main reasons for rejection, could be avoided.
Stem cells can be useful for several areas of interest such as drug development or development studies.
Finding a suitable stem cell source is the first step. Finding, isolating, and cultivating the proper type of stem cell, such as a rare cell in adult tissue, requires painstaking work.
Tissue-specific stem cells are thought to be less adaptable than embryonic and foetal stem cells, in general. The correct environment must be created after the stem cells have been identified and separated, an environment where the cells can differentiate into the specialized cells needed for a specific therapy.
A transport/migration system for cells to the area of the body where they are to act must be created. It is only in this area that the cells must perform their action, integrating with the body’s native cells. However, although cells can chemically recognize injured tissue, there may be a physical barrier, such as a blocked artery, preventing these cells from “traveling” to damaged regions. The rate of tissue regeneration will be poor, slow, or non-existent if the root cause of the blockage is not removed.
Like organ transplants, it may be necessary to suppress the immune system of the body to lessen the immune response triggered by the donated cells. It should be considered that the body may react negatively to the addition of progenitor cells causing the formation of tumors or accelerating their growth rate. The oncological field is, without a doubt, a field in which cell therapy research must be strengthened, given its potential, but with the appropriate measures.
Since 2001, hundreds of stem cell lines have been developed; these lines are much more adaptable and easier to deal with than lines established nearly a decade ago [70]. They also have the advantage of not being “contaminated” by being produced from other cells. Therefore, the National Institutes of Health (NIH) or other competitive funding organizations are unlikely to support experiments limited to older cell lines, given the advantages of newer ones [71]. The study of stem cells and their potential uses for the treatment of various human diseases is still in its infancy, despite encouraging results from animal models. To guarantee long-term efficacy and safety, a thorough research process should be followed.
7. Conclusion and final considerations
Fundamental knowledge of how organisms grow and develop, as well as how tissues are maintained throughout adult life, is aided by stem cell research. Understanding what goes wrong during disease and damage and, ultimately, how to treat these diseases, is necessary. In the future, researchers will have the means to simulate diseases, test medications, and create increasingly effective treatments with the help of developing human tissue and stem cell lines, and related biological products.
In conclusion, there are two factors that make the creation of disease- or patient-specific pluripotent stem cells extremely therapeutically promising. First, these cells may offer a powerful new tool for researching the causes of human diseases and for developing new drugs. Secondly, the generated ESCs could be transformed into a specific cell type and, if transplanted into the original donor, would be recognized as “autologous,” eliminating the issues with immunosuppression and rejection that arise with transplants from unrelated donors. The research must go on and unlock the potential of stem cells to further advance regenerative medicine.
Acknowledgments
We gratefully acknowledge the Department of Pathology and Diagnostics at the University of Verona, which allow to perform research.
Thanks
To Natasha, who in her modest comprehension of things knows how to pique my curiosity about the areas of my life that have not yet been thoroughly explored.
Thanks to all my dearest supporters who in the dark moment know how to encourage and spur me to work more and more. I would also like to thank all dear colleagues in the Department of Diagnostics and Public Health for providing knowledge and insights into some of the considerations in the chapter.
A special thanks to Sheila who took care to correct and revise the chapter several times, leaving no mistakes.
Special thanks to the IntechOpen Team for giving me the opportunity to write this chapter.
References
- 1.
Mahla RS. Stem cells applications in regenerative medicine and disease therapeutics. International Journal of Cell Biology. 2016; 2016 :e6940283. DOI: 10.1155/2016/6940283 - 2.
Stoltz J-F, de Isla N, Li YP, Bensoussan D, Zhang L, Huselstein C, et al. Stem cells and regenerative medicine: Myth or reality of the 21th century. Stem Cells International. 2015; 2015 :e734731. DOI: 10.1155/2015/734731 - 3.
Haseltine WA. The emergence of regenerative medicine: A new field and a new society. e-biomed: The Journal of Regenerative Medicine. 2001:17-23. DOI: 10.1089/152489001753309652 - 4.
Hyun I. The bioethics of stem cell research and therapy. The Journal of Clinical Investigation. 2010; 120 (1):71-75. DOI: 10.1172/JCI40435 - 5.
Cofano F, Boido M, Monticelli M, Zenga F, Ducati A, Vercelli A, et al. Mesenchymal stem cells for spinal cord injury: Current options, limitations, and future of cell therapy. International Journal of Molecular Sciences. 2019; 20 (11):2698. DOI: 10.3390/ijms20112698 - 6.
Totipotent Stem Cell-An overview Science Direct Topics. (s.d.). Recuperato 21 gennaio 2023, da. Available from: https://www.sciencedirect.com/topics/medicine-and-dentistry/totipotent-stem-cell - 7.
Paige CJ, Kincade PW, Shinefeld LA, Sato VL. Precursors of murine B lymphocytes. Physical and functional characterization, and distinctions from myeloid stem cells. Journal of Experimental Medicine. 1981; 153 (1):154-165. DOI: 10.1084/jem.153.1.154 - 8.
Nichols J, Zevnik B, Anastassiadis K, Niwa H, Klewe-Nebenius D, Chambers I, et al. Formation of pluripotent stem cells in the mammalian embryo depends on the POU transcription factor Oct4. Cell. 1998; 95 (3):379-391. DOI: 10.1016/S0092-8674(00)81769-9 - 9.
de Wert G, Mummery C. Human embryonic stem cells: Research, ethics and policy. Human Reproduction. 2003; 18 (4):672-682. DOI: 10.1093/humrep/deg143 - 10.
Adashi EY, Cohen IG. Who will oversee the ethical limits of human embryo research? Nature Biotechnology. 2022; 40 (4):463-464. DOI: 10.1038/s41587-022-01274-6. PMID: 35361998 - 11.
Kim C. Disease modeling and cell based therapy with iPSC: Future therapeutic option with fast and safe application. Blood Research. 2014; 49 (1):7. DOI: 10.5045/br.2014.49.1.7 - 12.
Steeg R, Mueller SC, Mah N, Holst B, Cabrera-Socorro A, Stacey GN, et al. EBiSC best practice: How to ensure optimal generation, qualification, and distribution of iPSC lines. Stem Cell Reports. 2021; 16 (8):1853-1867. DOI: 10.1016/j.stemcr.2021.07.009 - 13.
Scesa G, Adami R, Bottai D. iPSC preparation and epigenetic memory: Does the tissue origin matter? Cells. 2021; 10 (6):Art 6. DOI: 10.3390/cells10061470 - 14.
Tukker AM, de Groot MWGDM, Wijnolts FMJ, Kasteel EEJ, Hondebrink L, Westerink R. Is the time right for in vitro neurotoxicity testing using human iPSC-derived neurons? ALTEX-Alternatives to Animal Experimentation. 2016; 33 (3):Art. 3. DOI: 10.14573/altex.1510091 - 15.
Knoepfler PS. Deconstructing stem cell Tumorigenicity: A roadmap to safe regenerative medicine. Stem Cells. 2009; 27 (5):1050-1056. DOI: 10.1002/stem.37 - 16.
Hong SG, Winkler T, Wu C, Guo V, Pittaluga S, Nicolae A, et al. Path to the clinic: Assessment of iPSC-based cell therapies In vivo in a nonhuman primate model. Cell Reports. 2014; 7 (4):1298-1309. DOI: 10.1016/j.celrep.2014.04.019 - 17.
Taguchi J, Yamada Y. In vivo reprogramming for tissue regeneration and organismal rejuvenation. Current Opinion in Genetics & Development. 2017; 46 :132-140. DOI: 10.1016/j.gde.2017.07.008 - 18.
Bongso A, Lee EH. Stem Cells: From Bench to Bedside. World Scientific; 2005 - 19.
Ramalho-Santos M, Willenbring H. On the origin of the term “stem cell”. Cell Stem Cell. 2007; 1 (1):35-38. DOI: 10.1016/j.stem.2007.05.013 - 20.
Rossant J. Stem cells from the mammalian blastocyst. Stem Cells. 2001; 19 (6):477-482. DOI: 10.1634/stemcells.19-6-477 - 21.
Bourne DA, Thomas RD, Bliley J, Haas G, Wyse A, Donnenberg A, et al. Amputation-site soft-tissue restoration using adipose stem cell therapy. Plastic and Reconstructive Surgery. 2018; 142 (5):1349. DOI: 10.1097/PRS.0000000000004889 - 22.
Lajtha LG. Stem cell concepts. Differentiation. 1979; 14 (1):23-33. DOI: 10.1111/j.1432-0436.1979.tb01007.x - 23.
Bonafede R, Turano E, Scambi I, Busato A, Bontempi P, Virla F, et al. ASC-exosomes ameliorate the disease progression in SOD1 (G93A) murine model underlining their potential therapeutic use in human ALS. International Journal of Molecular Sciences. 2020; 21 (10):art. 10. DOI: 10.3390/ijms21103651 - 24.
Busato A, Bonafede R, Bontempi P, Scambi I, Schiaffino L, Benati D, et al. Magnetic resonance imaging of ultrasmall superparamagnetic iron oxide-labeled exosomes from stem cells: A new method to obtain labeled exosomes. International Journal of Nanomedicine. 2016; 11 :2481-2490. DOI: 10.2147/IJN.S104152 - 25.
Busato A, Bonafede R, Bontempi P, Scambi I, Schiaffino L, Benati D, et al. Labeling and magnetic resonance imaging of exosomes isolated from adipose stem cells. Current Protocols in Cell Biology. 2017; 75 (1):3.44.1-3. 44.15. DOI: 10.1002/cpcb.23 - 26.
Kolios G, Moodley Y. Introduction to stem cells and regenerative medicine. Respiration. 2013; 85 (1):3-10. DOI: 10.1159/000345615 - 27.
Clevers H. What is an adult stem cell? Science. 2015; 350 (6266):1319-1320. DOI: 10.1126/science.aad7016 - 28.
Young HE, Black AC Jr. Adult stem cells. The Anatomical Record Part A: Discoveries in Molecular, Cellular, and Evolutionary Biology. 2004; 276A (1):75-102. DOI: 10.1002/ar.a.10134 - 29.
Barker N, Bartfeld S, Clevers H. Tissue-resident adult stem cell populations of rapidly self-renewing organs. Cell Stem Cell. 2010; 7 (6):656-670. DOI: 10.1016/j.stem.2010.11.016 - 30.
Schepers A, Clevers H. Wnt signaling, stem cells, and cancer of the gastrointestinal tract. Cold Spring Harbor Perspectives in Biology. 2012; 4 (4):a007989. DOI: 10.1101/cshperspect.a007989 - 31.
Ikehara S. Grand challenges in stem cell treatments. Frontiers in Cell and Developmental Biology. 2013; 1 :2 - 32.
Serakinci N, Keith WN. Therapeutic potential of adult stem cells. European Journal of Cancer. 2006; 42 (9):1243-1246. DOI: 10.1016/j.ejca.2006.01.036 - 33.
What is an adult stem cell? Science. (s.d.). Recuperato 20 gennaio 2023, da. Available from: https://www.science.org/doi/full/10.1126/science.aad7016 - 34.
Alison M, Islam S. Attributes of adult stem cells. The Journal of Pathology. 2009; 217 (2):144-160. DOI: 10.1002/path.2498 - 35.
De Francesco F, Gravina P, Busato A, Farinelli L, Soranzo C, Vidal L, et al. Stem cells in autologous microfragmented adipose tissue: Current perspectives in osteoarthritis disease. International Journal of Molecular Sciences. 2021a; 22 (19):art. 19. DOI: 10.3390/ijms221910197 - 36.
De Francesco F, Matta C, Riccio M, Sbarbati A, Mobasheri A. Reevolution of tissue regeneration: From recent advances in adipose stem cells to novel therapeutic approaches. Stem Cells International. 2021b; 2021 :e2179429. DOI: 10.1155/2021/2179429 - 37.
Bonafede R, Brandi J, Manfredi M, Scambi I, Schiaffino L, Merigo F, et al. The anti-apoptotic effect of ASC-exosomes in an In vitro ALS model and their proteomic analysis. Cells. 2019; 8 (9):art. 9. DOI: 10.3390/cells8091087 - 38.
Exosomes: Immune properties and potential clinical implementations SpringerLink. (s.d.). Recuperato 7 gennaio 2023, da. Available from: https://link.springer.com/article/10.1007/s00281-010-0233-9 - 39.
Xiong M, Zhang Q , Hu W, Zhao C, Lv W, Yi Y, et al. Exosomes from adipose-derived stem cells: The emerging roles and applications in tissue regeneration of plastic and cosmetic surgery. Frontiers in Cell and Developmental Biology. 2020; 8 :574223 - 40.
Rippon HJ, Bishop AE. Embryonic stem cells. Cell Proliferation. 2004; 37 (1):23-34. DOI: 10.1111/j.1365-2184.2004.00298.x - 41.
Waldby C. Oocyte markets: Women’s reproductive work in embryonic stem cell research. New Genetics and Society. 2008; 27 (1):19-31. DOI: 10.1080/14636770701843576 - 42.
Odorico JS, Kaufman DS, Thomson JA. Multilineage differentiation from human embryonic stem cell lines. Stem Cells. 2001; 19 (3):193-204. DOI: 10.1634/stemcells.19-3-193 - 43.
Keller G. Embryonic stem cell differentiation: Emergence of a new era in biology and medicine. Genes & Development. 2005; 19 (10):1129-1155. DOI: 10.1101/gad.1303605 - 44.
Elisseeff JH. Embryonic stem cells: Potential for more impact. Trends in Biotechnology. 2004; 22 (4):155-156. DOI: 10.1016/j.tibtech.2004.02.006 - 45.
Menasché P. Human embryonic stem cells still have a place in the cell therapy landscape. Cardiovascular Research. 2022; 118 (13):e96-e97. DOI: 10.1093/cvr/cvac117 - 46.
Cherry ABC, Daley GQ. Reprogrammed cells for disease modeling and regenerative medicine. Annual Review of Medicine. 2013; 64 :277-290. DOI: 10.1146/annurev-med-050311-163324 - 47.
Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006; 126 (4):663-676. DOI: 10.1016/j.cell.2006.07.024 - 48.
Malik N, Rao MS. A review of the methods for human iPSC derivation. In: Lakshmipathy U, Vemuri MC (A c. Di). Pluripotent Stem Cells: Methods and Protocols. Humana Press; 2013. pp. 23-33. DOI:10.1007/978-1-62703-348-0_3 - 49.
Wiegand C, Banerjee I. Recent advances in the applications of iPSC technology. Current Opinion in Biotechnology. 2019; 60 :250-258. DOI: 10.1016/j.copbio.2019.05.011 - 50.
Nicholson MW, Ting C-Y, Chan DZH, Cheng Y-C, Lee Y-C, Hsu C-C, et al. Utility of iPSC-derived cells for disease modeling, drug development, and cell therapy. Cells. 2022; 11 (11):Art. 11. DOI: 10.3390/cells11111853 - 51.
MacArthur CC, Pradhan S, Switalski S, Landon M, Lakshmipathy U. Establishing iPSC cell banks derived using reagents and workflows optimized for cell therapy manufacturing. Cytotherapy. 2019; 21 (5 Supplement):S13. DOI: 10.1016/j.jcyt.2019.03.574 - 52.
Körbling M, Estrov Z. Adult stem cells for tissue repair—A new therapeutic concept? New England Journal of Medicine. 2003; 349 (6):570-582. DOI: 10.1056/NEJMra022361 - 53.
Squillaro T, Peluso G, Galderisi U. Clinical trials with mesenchymal stem cells: An update. Cell Transplantation. 2016; 25 (5):829-848. DOI: 10.3727/096368915X689622 - 54.
Meisner LF, Johnson JA. Protocols for cytogenetic studies of human embryonic stem cells. Methods. 2008; 45 (2):133-141. DOI: 10.1016/j.ymeth.2008.03.005 - 55.
Pouton CW, Haynes JM. Embryonic stem cells as a source of models for drug discovery. Nature Reviews Drug Discovery. 2007; 6 (8):Art. 8. DOI: 10.1038/nrd2194 - 56.
Tamm C, Galitó SP, Annerén C. A comparative study of protocols for mouse embryonic stem cell culturing. PLoS One. 2013; 8 (12):e81156. DOI: 10.1371/journal.pone.0081156 - 57.
Turksen K. Embryonic Stem Cells: Methods and Protocols. Springer Science & Business Media; 2008 - 58.
Appelt-Menzel A, Oerter S, Mathew S, Haferkamp U, Hartmann C, Jung M, et al. Human iPSC-derived blood-brain barrier models: Valuable tools for preclinical drug discovery and development? Current Protocols in Stem Cell Biology. 2020; 55 (1):e122. DOI: 10.1002/cpsc.122 - 59.
Harding J, Mirochnitchenko O. Preclinical studies for induced pluripotent stem cell-based therapeutics *. Journal of Biological Chemistry. 2014; 289 (8):4585-4593. DOI: 10.1074/jbc.R113.463737 - 60.
van Amerongen RA, Morton LT, Chaudhari UG, Remst DFG, Hagedoorn RS, van den Berg CW, et al. Human iPSC-derived preclinical models to identify toxicity of tumor-specific T cells with clinical potential. Molecular Therapy-Methods & Clinical Development. 2023; 28 :249-261. DOI: 10.1016/j.omtm.2023.01.005 - 61.
Chiu RC-J. Bone-marrow stem cells as a source for cell therapy. Heart Failure Reviews. 2003; 8 (3):247-251. DOI: 10.1023/A:1024769617018 - 62.
Kim JY, Nam Y, Rim YA, Ju JH. Review of the current trends in clinical trials involving induced pluripotent stem cells. Stem Cell Reviews and Reports. 2022; 18 (1):142-154. DOI: 10.1007/s12015-021-10262-3 - 63.
Menon A, Vijayavenkataraman S. Novel vision restoration techniques: 3D bioprinting, gene and stem cell therapy, optogenetics, and the bionic eye. Artificial Organs. 2022; 46 (8):1463-1474. DOI: 10.1111/aor.14241 - 64.
Stocum DL, Zupanc GKH. Stretching the limits: Stem cells in regeneration science. Developmental Dynamics. 2008; 237 (12):3648-3671. DOI: 10.1002/dvdy.21774 - 65.
Capuzzo AM, Vigo D. Microfluidic live-imaging technology to perform research activities in 3D models. 2021. Available from: https://www.researchgate.net/publication/349923987_Microfluidic_Live-Imaging_Technology_to_Perform_Research_Activities_in_3D_Models - 66.
Capuzzo AM, Vigo D. Updated modifications about spin∞ bioreactor. Journal of Engineering Technology and Applied Sciences. 2020; 5 :53-56 - 67.
Findikli N, Candan N, Kahraman S. Human embryonic stem cell culture: Current limitations and novel strategies. Reproductive Biomedicine Online. 2006; 13 (4):581-590. DOI: 10.1016/S1472-6483(10)60648-7 - 68.
Murry CE, Keller G. Differentiation of embryonic stem cells to clinically relevant populations: Lessons from embryonic development. Cell. 2008; 132 (4):661-680. DOI: 10.1016/j.cell.2008.02.008 - 69.
All Roads Lead to Induced Pluripotent Stem Cells: The Technologies of iPSC Generation Stem Cells and Development. (s.d.). Recuperato 7 gennaio 2023, da. Available from: https://www.liebertpub.com/doi/full/10.1089/scd.2013.0620 - 70.
Bongso A, Richards M. History and perspective of stem cell research. Best Practice & Research Clinical Obstetrics & Gynaecology. 2004; 18 (6):827-842. DOI: 10.1016/j.bpobgyn.2004.09.002 - 71.
Tagle DA. The NIH microphysiological systems program: Developing in vitro tools for safety and efficacy in drug development. Current Opinion in Pharmacology. 2019; 48 :146-154. DOI: 10.1016/j.coph.2019.09.007